
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Spectral computed tomography (SCT) after cardiovascular electronic devices implantation: No more blinding lights
Franceschi P; Russo V*; Lovato L
Pediatric and Adult CardioThoracic and Vascular, Oncohematologic and Emergency Radiology Unit, IRCCS University Hospital of Bologna, Via Massarenti 9, 40138, Bologna, BO, Italy.
*Corresponding Author : Vincenzo Russo
Pediatric and Adult CardioThoracic and Vascular, Oncohematologic and Emergency Radiology Unit, IRCCS University Hospital of Bologna, Via Massarenti 9, 40138, Bologna, BO, Italy.
Email: vincenzo.russo@aosp.bo.it
Received : Apr 22, 2024
Accepted : May 09, 2024
Published : May 16, 2024
Archived : www.jcimcr.org
Copyright : © Russo V (2024).
Abstract
Accurate localization of intraventricular electrode tips in patients with Cardiac Implantable Electronic Devices (CIEDs) remains a challenge, necessitating advanced imaging techniques. Traditional methodologies, such as Chest X-ray (CXR) and echocardiography, may prove insufficient in precisely determining electrode positions. ECG-gated contrast enhanced coronary Computed Tomography (CT) angiography provides the clearest assessment of lead position relative to the myocardium but its effectiveness can be seriously compromised by metallic artifacts. In this scenario, Spectral Computed Tomography (SCT) imaging stands out as a promising solution, offering artifact reduction and enhanced tissue contrast, in particular with “iodine no water” images. In this report, we present a compelling case that highlights the effectiveness of DECT in precisely locating an intraventricular electrode tip, thereby illustrating its potential value in clinical practice. Our findings advocate for the integration of SCT into the diagnostic algorithm for comprehensive cardiac device management, facilitating non-invasive patient follow-up and minimizing the need for additional and invasive procedures.
Keywords: Spectral CT imaging; Material decomposition; Iodine no water; Virtual monoenergetic images; Cardiac Implantable Electronic Devices (CIEDs).
Abbreviations: CIEDs: Cardiac Implantable Electronic Devices; CT: Computed Tomography; CXR: Chest X-Ray; SCT: Spectral CT; ECG: Electrocardiogram; PM: Pace Maker.
Citation: Franceschi P, Russo V, Lovato L. Spectral computed tomography (SCT) after cardiovascular electronic devices implantation: No more blinding lights. J Clin Images Med Case Rep. 2024; 5(5): 3056.
Introduction
Accurate localization of intraventricular electrode tips in patients with Cardiac Implantable Electronic Devices (CIEDs) poses a persistent challenge, necessitating the application of advanced imaging techniques [1]. Traditional methodologies, such as Chest X-ray (CXR) and echocardiography, often prove insufficient in precisely determining electrode positions, particularly in cases of heightened complexity. Despite recent strides in enhancing the compatibility of cardiac devices with magnetic resonance imaging, metallic artifacts persist, greatly limiting the role of this modality in this clinical setting. ECG-gated contrast enhanced coronary Computed Tomography (CT) angiography provides the clearest assessment of lead position relative to the myocardium and also demonstrate concurrent complications (pleural effusion, pneumothorax, or unusual extracardiac migration pf the leads) but its effectiveness can be compromised by metallic artifacts [2-5]. In this context, Spectral Computed Tomography (SCT) emerges as a promising avenue, providing artifact reduction and heightened tissue contrast [6]. Herein, we present a compelling case underscoring the efficacy of SCT in accurately localizing an intraventricular electrode tip, thereby shedding light on its potential within clinical practice.
Case report
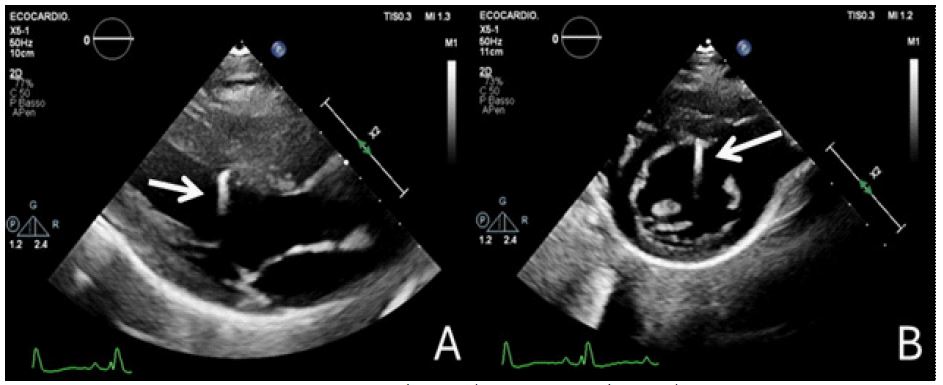
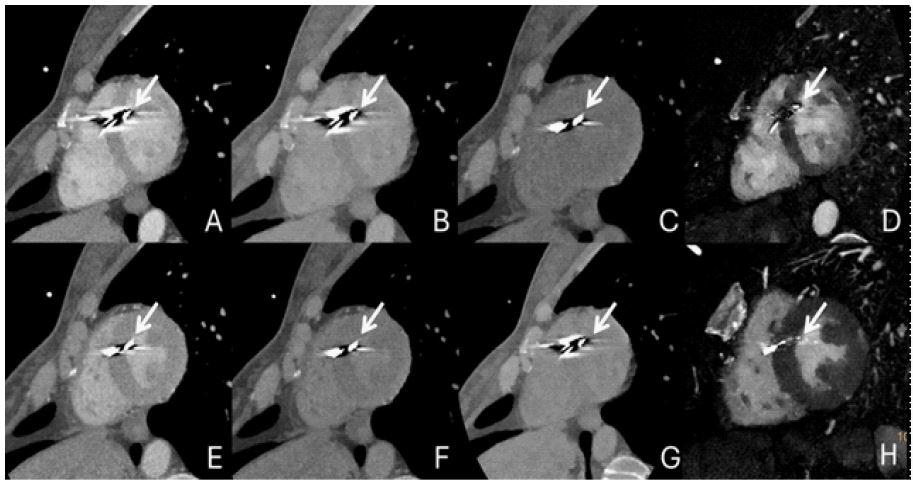
We report a case of a woman in her forties who underwent permanent bicameral Pacemaker (PM) implantation following third-degree atrioventricular block detection on electrocardiogram. Right ventricular and atrial leads were inserted via extra-thoracic left subclavian vein puncture due to cephalic vein inaccessibility. The PM was subcutaneously positioned in a left subclavian pocket without immediate post-procedural complications. Subsequent follow-ups revealed the patient’s asymptomatic and stable health status. However, echocardiography raised concerns regarding a possible left intraventricular displacement of the distal end of the right ventricular “septal” lead, warranting further investigation (Figure 1). Electrophysiological assessments indicated consistent device function. To enhance lead tip visualization, ECG-gated contrast enhanced coronary CT angiography was performed using a Philips 7500 Spectral dual-layer scanner. On conventional images, even using 140 kV we were not able to localize the distal end of the ventricular catheter due to metallic artifacts. Spectral CT technology allowed “Iodine no water” reconstructions which suggested the lead tip was just pressing against the septal wall, without perforation (Figure 2). Integration of CT findings with electrophysiological data guided the decision for non-invasive follow-up as the optimal patient management strategy.
Discussion/Conclusion
This case emphasizes the enhanced utility of SCT imaging in managing complications following the implantation of CIEDs attributable to mechanical factors (e.g., cardiac perforation and tamponade), where the identification of the leads’ tips is imperative [1]. These complications are rare but potentially life-threatening. They usually happen acutely, at the time of lead insertion, but may also occur several months or years following implantation. Clinical presentation is highly variable - from asymptomatic cases with loss of lead capture to chest pain, dyspnea, and cardiac tamponade. Clinical and imaging patient monitoring after invasive procedures is mandatory. The selection of the most appropriate imaging modalities will depend on the clinical circumstances and the suspected complication. CXR or echocardiography are the initial imaging modalities of choice in most cases, but they may lack the sensitivity required for precise intraventricular electrode localization. ECG-gated contrast enhanced coronary CT angiography provides the clearest assessment of lead position relative to the myocardium and also demonstrate concurrent complications (pleural effusion, pneumothorax, or unusual extracardiac migration of the leads) but its effectiveness can be compromised by metallic artifacts [2-5]. In this context, SCT thanks to material decomposition techniques provides artifact reduction and improved tissue contrast, enabling accurate lead localization without invasive interventions [6]. Among the reconstructions enabled by spectral CT technology, high keV VMI are recommended for reducing metallic artifacts. However, in our case, increasing the keV mitigated metallic artifacts originating from the lead’s body but not those arising from its tip due to the different composition of the structures. Furthermore, high keV VMI decreased tissue contrast, making it difficult to differentiate the septal myocardium surrounding the lead’s tip from the left ventricular blood pool, even after contrast agent administration. This hindered the localization of the lead’s tip, preventing the exclusion of its migration into the left ventricle. However, “Iodine no water” images allowed for the best differentiation among the three materials: metal, myocardium, and blood pool. In fact, in these images, metallic artifacts generated by the lead’s tip were minimized, facilitating the accurate identification of the lead itself. Additionally, tissue contrast was enhanced, improving the distinction between myocardium and blood pool. Our findings advocate for the integration of SCT into the diagnostic algorithm for comprehensive cardiac device management and patient monitoring after cardiac device implantation, facilitating non-invasive patient follow-up and minimizing the need for additional and invasive procedures.
References
- Stankovic I, Voigt JU, Burri H, Muraru D, Sade LE, Haugaa KH, et al. Imaging in patients with cardiovascular implantable electronic devices: part 2-imaging after device implantation. A clinical consensus statement of the European Association of Cardiovascular Imaging (EACVI) and the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J Cardiovasc Imaging. 21 dicembre. 2023; 25(1): 33-54.
- Voros S. What are the potential advantages and disadvantages of volumetric CT scanning? J Cardiovasc Comput Tomogr. marzo. 2009; 3(2): 67-70.
- Smolka S, Achenbach S. Koronare Computertomographie bei Device-Trägern: Sinnvolle Diagnostik oder nur Artefakt? Herzschrittmachertherapie Elektrophysiologie. settembre 2022; 33(3): 283-9.
- Li Q, Dai W, Fang D, Ma W, Lin C, Lu C, et al. Occurrence of ventricular septal perforation in patients with permanent left bundle branch pacing followed up using echocardiographic and computed tomography images. Ann Noninvasive Electrocardiol. 10 settembre. 2022; 27(6): 13002.
- Reinartz SD, Kuhl CK, Fehrenbacher K, Napp A. Magic Angle in Cardiac CT: Eliminating Clinically Relevant Metal Artifacts in Pacemaker Leads with a Lead-Tip/Gantry Angle of ≤70°. Acad Radiol. 1 luglio. 2018; 25(7): 898-903.
- Selles M, Van Osch JAC, Maas M, Boomsma MF, Wellenberg RHH. Advances in metal artifact reduction in CT images: A review of traditional and novel metal artifact reduction techniques. Eur J Radiol. gennaio. 2024; 170: 111276.