
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Optic disc visualization through silicone oil behind the crystalline lens
Arnav Panigrahi*; Abhishek Singh; Shikha Gupta; Viney Gupta
Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
*Corresponding Author : Arnav Panigrahi
Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
Email: arnav.888panigrahi@gmail.com
Received : Apr 17, 2024
Accepted : May 10, 2024
Published : May 17, 2024
Archived : www.jcimcr.org
Copyright : © Panigrahi A (2024).
Abstract
Silicone oil (SO) is used as a vitreous tamponade, because of its non-immunogenic and inert properties as well as the transparency it permits for posterior segment evaluation without inducing any aberration [1]. However, the emulsified SO can obscure a proper fundus visualization, though such observations have not been explicitly published. Here we present a case where dispersed emulsified SO bubbles, clinging to the posterior surface of crystalline lens, caused distortions in fundus imaging and hampered with optic disc visualization.
Citation: Panigrahi A, Singh A, Gupta S, Gupta V. Optic disc visualization through silicone oil behind the crystalline lens. J Clin Images Med Case Rep. 2024; 5(5): 3058
Case Report
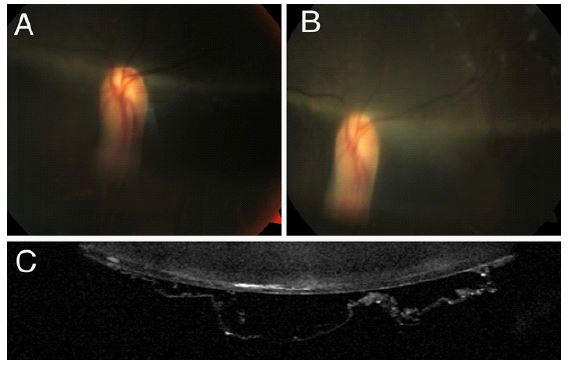
Two unrelated adults, with history of vitreoretinal surgery with silicone oil (SO) tamponade, presented with elevated intraocular pressure in the operated eye, 3 months post SO removal. The media was clear but optic disc image was found to be distorted despite all manoeuvres to visualise it. In both the cases, a white ridge could be seen passing through the superior half of the optic disc, with the inferior half appearing blurred and elongated, thereby precluding disc assessment (Figure 1A,1B). SO bubbles could be seen behind the crystalline lens in both of them (Figure 1C).
Discussion
It is known that SO in the vitreous cavity leads not only to changes in low-order aberrations (spherical or cylindrical error) but also to changes in high-order aberrations [2,3]. The SO droplets can stick to the silicone intraocular lens due to adhesive force between their similar molecules [4]. SO filled eye is known to cause total internal reflection of laser light [5]. In the crystalline lens, the posterior curvature and refractive index of the lens increase from the periphery toward the centre, resulting in peripheral rays from the object when focusing behind the plane in which the central rays focus with the intraocular SO. This can lead to larger aberrations with SO tamponade in phakic than pseudophakic eyes. In our case, the emulsified SO droplets were adherent to the posterior surface of the crystalline lens, hampering fundus visualization and also causing visual disturbance to the patient, probably due to internal reflections of light. The presence of such SO droplets should be looked for in eyes that have undergone vitreoretinal surgery with SO tamponade and present with difficult visualization of fundus details. Such an aberration makes clinical assessment of a glaucomatous disc difficult, hence hampering decision-making. In such vitrectomized eyes where disc assessment is not possible, visual field assessment thus becomes paramount for optimal management of glaucoma.
References
- Chen Y, Kearns VR, Zhou L, et al. Silicone oil in vitreoretinal surgery: indications, complications, new developments and alternative long-term tamponade agents. Acta Ophthalmol. 2021; 99: 240-250.
- McCuen BW 2nd, de Juan E Jr, Landers MB 3rd, Machemer R. Silicone oil in vitreoretinal surgery. Part 2: Results and complications. Retina. 1985; 5: 198-205.
- Shin JY, Chung IK, Han GH, et al. Higher-Order Aberrations in Eyes With Silicone Oil Tamponade. Retina. 2020; 40: 735-742.
- Hu CL, Peng KL. Removal of silicone oil droplets adhering to the posterior surface of an intraocular lens (IOL). Int Med Case Rep J. 2018; 11: 157-159.
- Bartov E, Rock T, Treister G, Belkin M. Total internal reflection of laser light in eyes filled with silicone oil. Ophthalmic Surg Lasers. 1999; 30: 17-23.