
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Systematic investigation: Prognostic and clinical significance of Hsp90aa1 in laryngeal cancer
Hong Chen; Panpan Xu; Wei Jin*
Department of Otolaryngology, Head and Neck Surgery, Chaohu Hospital Affiliated to Anhui Medical University, Chaohu 238000, China.
*Corresponding Author : Wei Jin
Department of Otolaryngology, Head and Neck Surgery,
Chaohu Hospital Affiliated to Anhui Medical
University, Chaohu 238000, China.
Email: 13965689458@163.com
Received : Apr 08, 2024
Accepted : May 14, 2024
Published : May 21, 2024
Archived : www.jcimcr.org
Copyright : © Jin W (2024).
Abstract
We performed expression analysis on the expression data of Laryngeal Cancer (LC) samples to determine the expression differences of HSP90AA1 in tumors and normal samples, and evaluated the methylation level, prognostic significance, functional pathways and risk significance of HSP90AA1, and obtained the results in LC. The important role of HSP90AA1 in the prognosis of LC patients. TCGA-LC data of LC were obtained from the TCGA database. Through differential expression analysis, we obtained the differential genes between the HSP90AA1 high-expression group and the low-expression group, and obtained the key biological pathways and biological processes through Gene Set Enrichment Analysis (GSEA) analysis. Further, based on clinical data, we analyzed the correlation between various indicators and HSP90a in LC patients from Anhui Medical University Affiliated Hospital. We used LC data in public databases to identify the importance of HSP90AA1 in the prognosis of LC patients, and analyzed the close correlation between HSP90AA1 and various indicators of LC based on clinical data. This may provide an effective basis for clinical precision treatment of LC.
Keywords: HSP90AA1; Laryngeal cancer; Gene set enrichment analysis; prognosis; Biomarker.
Abbreviation: LC: Laryngeal Cancer; GSEA: Gene Set Enrichment Analysis; HSP90: Heat Shock Protein 90; TCGA: The Cancer Genome Atlas; GO: Gene Ontology; OS: Overall Survival; DSS: Disease-Free Survival; PFS: Progression-Free Survival.
Citation: Chen H, Xu P, Jin W. Systematic investigation: Prognostic and clinical significance of Hsp90aa1 in laryngeal cancer. J Clin Images Med Case Rep. 2024; 5(5): 3063.
Introduction
Laryngeal Cancer (LC) is a common malignant tumor of the upper respiratory tract. Although the current treatment methods such as surgery, radiotherapy and chemotherapy have improved the efficacy of patients with early LC, the prognosis of patients with advanced LC is still not optimistic [1]. Therefore, revealing the potential biomarkers of LC is crucial for exploring effective treatment strategies [2]. Heat Shock Protein 90 (HSP90) is an important chaperone protein, which regulates the signal pathway and corrects the misfolded proteins in cancer cells by interacting with oncogenic client proteins and co-chaperone proteins [3]. The inhibition of HSP90 molecular chaperone mechanism has been proved to be a potential way to inhibit tumor survival, proliferation, invasion and migration [4]. The role of HSP90 in the prognosis of LC is still unclear and needs to be studied [5].
Higher levels of HSP90AA1 transcription and expression and activity of the AKT1/ERK pathway have been confirmed in studies of other cancer patients. In human and mouse lung cancer cell lines, knockdown of HSP90AA1 promotes apoptosis by reducing the phosphorylation of itself and its downstream factors mTOR and BAD, as well as downregulating Mcl1, Bcland inhibiting the pro-survival effects of AKT1. XL and survival. This knockdown also inhibited laryngeal cancer cell proliferation by inhibiting ERK activation and downregulating CyclinD1 expression [6]. Treatment with the HSP90 inhibitor 17-DMAG recapitulated these effects in vitro, inhibited tumor cell growth and induced apoptosis in a lung tumor xenograft mouse model without apparent side effects. This study suggests that targeting HSP90 with may be a potential therapy for the treatment of laryngeal cancer [7].
Therefore, in this work, we evaluated the significance of HSP90AA1 gene expression patterns, prognostic value, functional pathways, and clinical data in LC by performing comprehensive bioinformatics analysis in several large online databases. These findings reveal the important role of HSP90AA1 in LC and identify potential therapeutic targets for LC [8].
Materials and methods
Data process: Open access data on transcriptional profiles and clinical characteristics were downloaded from The Cancer Genome Atlas (TCGA) database. The initial expression profiles (STAR-Counts form) of LC patients were organized into a combination matrix (TPM form) for subsequent analysis. We extracted survival and clinical information based on the bcr-xml file in TCGA-LC. Pan-cancer expression data are from UCSC Xena website (https://xenabrowser.net/) [9]. The limma and affay packages in the R environment were used for data preprocessing, including background correction, probe ID annotation, missing value completion and normalization [10]. Open access LC immunohistochemistry images from the Human Protein Atlas database [11]. For further exploring the prognostic role of clusters, univariate regression analysis was also performedto filter the significant prognostic factors [12].
Differential expression analysis and enrichment analysis: Use the limma package in the R environment to perform DEG analysis under specific parameters and visualize by using ggplot. Clusterprofiler in R was used to enrich Gene Ontology (GO) terms. Gene Set Enrichment Analysis (GSEA) was used to study potential biological differences between two selected groups based on set reference gene sets, including the Hallmark gene set [13]. Functional enrichment analysis was performed by converting gene names into gene IDs using the R package org. Hs. e.g., db [14]. Gene Ontology (GO) of DEGs and the Kyoto Encyclopedia of Genes and Genomes were analyzed using the R package clusterProfiler. Significantly different GO projects and signaling pathways were screened by a threshold P value of 0.05 and a threshold q value of 0.05 [15]. Results were visualized using the R package enrichment plots and ggplot2 [16].
Prognostic nomogram construction: To further explore the prognostic role of clustering, univariate regression analysis was also performed to screen for significant prognostic factors. To determine which clusters were significantly associated with OS, a univariate regression model was used and p values were calculated. Gene classifier features with a p value< 0.05 were significantly associated with clinicopathological features. Subsequently, a prognostic nomogram was constructed by combining significant features derived from multiple regression analysis with survival and RMS packages to improve the predictive powpower. Calibration plots are commonly used charts for assessing the consistency of nomograms and were generated using the rms package of R software [14].
Clinical data collection: Analyze 90 cases of laryngeal cancer patients who underwent surgical treatment at Chaohu Hospital of Anhui Medical University from January 2017 to December 2022 and were classified into the observation group; all patients were clearly diagnosed with laryngeal cancer by pathological examination.
Inclusion criteria for laryngeal cancer patients: (1) Diagnosed with laryngeal cancer for the first time through pathology, imaging, clinical signs and other examinations, and the pathological type has been clarified; (2) Not receiving surgery, antitumor drugs and radiotherapy; (3) Not combined with other diseases Tumor; (4) There are no serious abnormalities in liver, kidney, and heart functions. (5) Have not taken any drugs that affect CEA, CA125, or SCC-Ag levels. Those who had a healthy physical examination showed no tumor disease, laryngeal disease, or heart disease. The collection of medical history data obtained informed consent from the patients and was reviewed by the Medical Ethics Committee.
CEA, CA125, and SCC-Ag detection: CEA, CA125, and SCC-Ag detection were performed in all patients before surgery [17]. 5 ml of peripheral venous blood was collected and uniformly sloshed, and stored at 2-8OC to ensure completion of detection within 24 h. All test kits were purchased from Shenzhen New Industry Biomedical Engineering Co., LTD. The detection method was chemiluminescence immunoassay. Add 10 ul standard products, quality control products and specimens into each test tube, add 40 ul luminescent label and 40 ul fluorescin label, mix well and put them in a water bath for 30 min, the temperature of the water bath is 37OC, add them in a magnetic separator for 4 min, remove the supernuant and add 400 ul washing solution, mix them well and put them in a magnetic separator for 4 min. Remove the supernatant and test on the machine. According to the normal reference value range of automatic chemiluminescence similar products, the normal reference value is 95% distribution.
Result
Whole-cancer analysis of HSP90AA1 and its clinical prognostic role in LC: The expression of HSP90AA1 is shown in Figure 1A, in which HSP90AA1 exhibits abnormal expression patterns in most cancers, indicating its important role in cancer development. According to TCGA data, HSP90AA1 showed higher expression levels in LC tumor tissues compared with control normal tissues (Figure 1A,B). Furthermore, according to the immunohistochemistry results of the HPA database, higher HSP90AA1 protein levels were observed in renal cancer tissues (Figure 1C). Furthermore, we sought to investigate the prognostic role of HSP90AA1 in LC. The results indicate that HSP90AA1 may be associated with poor prognostic performance in LC patients, including Overall Survival (OS), Disease-Free Survival (DSS), and Progression-Free Survival (PFS) in the TCGA cohort (Figure 1D,F). We then explored the clinical relevance of HSP90AA1 in LC patients. There were obvious differences in the expression of HSP90AA1 in patients with different Stage classifications (Figure 1G). Based on univariate analysis, HSP90AA1 was an independent risk factor for LC (Figure 1H).
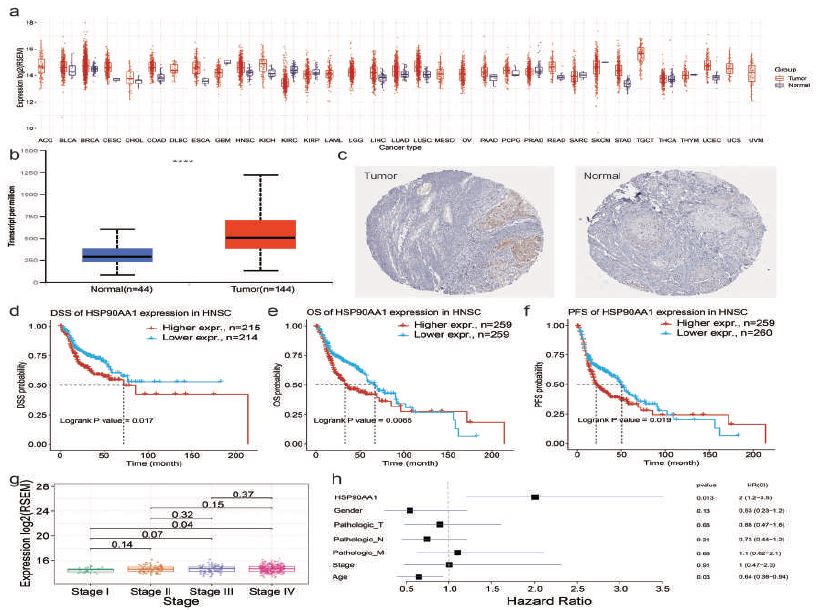
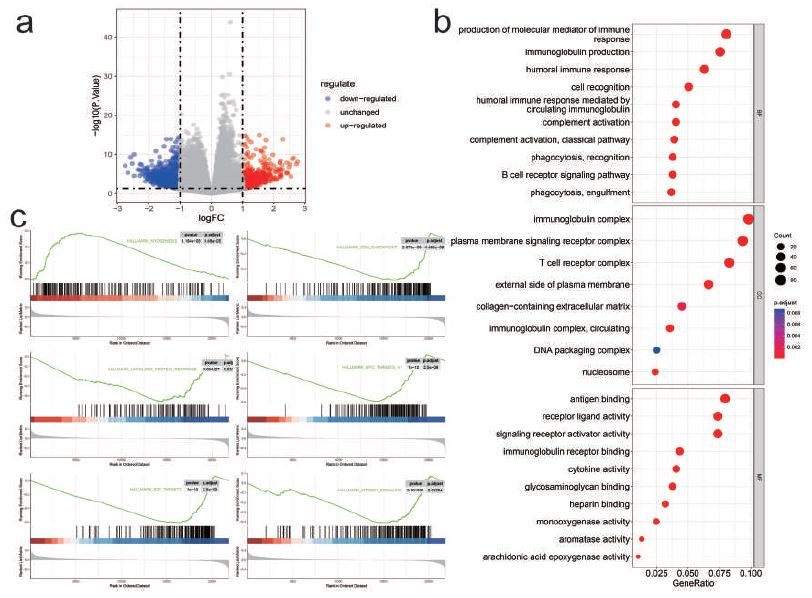
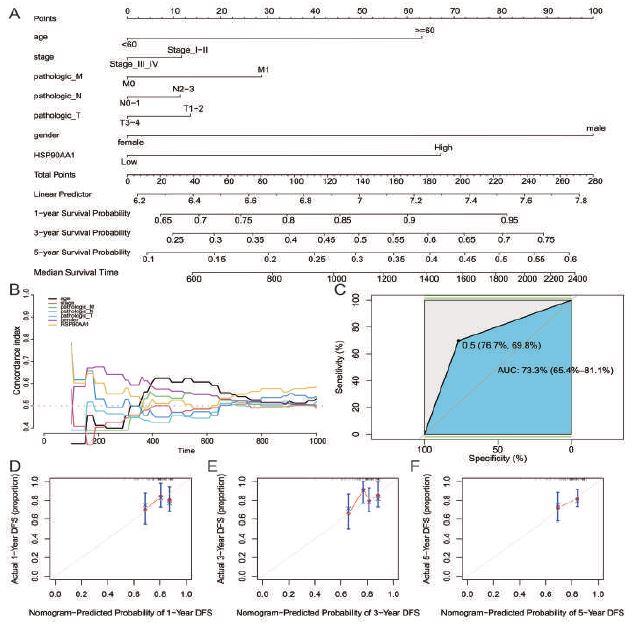
Table 1: Comparison of sample data among three groups.
| Group | Counts | Gender | Age | Bodymass index> (kg/m>2) | Smoking history[n(%)] | Drinking history> [n(%)] | |||
|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Smoking history | No> history ofsmoking | Smoking history | No history of drinking | ||||
| Laryngeal cancergroup | 89 | 49 (55.06) | 40 (44.94) | 62.64±8.12 | 21.30±2.28 | 42 (47.19) | 47 (52.81) | 46 (51.69) | 43 (48.31) |
| Laryngeal> vocal cord benigntumor group | 82 | 48 (58.54) | 34 (41.46) | 61.39±6.58 | 21.75±1.60 | 39 (47.56) | 43 (52.44) | 46 (56.10) | 36 (43.90) |
| Control group | 70 | 37 (52.86) | 33 (47.14) | 62.39±6.79 | 21.19±2.37 | 38 (54.29) | 32 (45.71) | 34 (48.57) | 36 (51.43) |
| χ2/F value | 0.510 | 0.691 | 1.570 | 0.953 | 0.878 | ||||
| Pvalue | 0.775 | 0.502 | 0.210 | 0.621 | 0.645 | ||||
Table 2: Comparison of plasma Hsp90a and tumor markers among the three groups.
| Group | Counts | Hsp90a (ng/mL) | CEA (ng/L) | SCC-Ag (ng/L) | CA199 (U/mL) |
|---|---|---|---|---|---|
| Laryngeal> cancergroup | 89 | 89.79±9.06 | 8.77±1.20 | 2.09±0.33 | 49.63±7.73 |
| Laryngeal> vocalcord> benign> tumorgroup | 82 | 58.04±6.10* | 5.13±0.64* | 1.90±0.25* | 15.57±2.17* |
| Control> group | 70 | 25.67±3.57*# | 3.76±0.33*# | 1.05±0.12*# | 7.88±0.81*# |
| Fvalue | 1731.102 | 775.209 | 347.754 | 1707.557 | |
| Pvalue | <0.001 | <0.001 | <0.001 | <0.001 |
Note: Compared with the normal control group, *P< 0.05; compared with the laryngeal vocal cord benign tumor group, #P< 0.05.
Table 3: Comparison of plasma Hsp90a and tumor markers in patients with different characteristics of laryngeal cancer.
| Clinical> factor | Type | counts | Plasma> Hsp90a (ng/mL) | CEA (ng/L) | SCC-Ag (ng/L) | CA199 (ng/L) |
|---|---|---|---|---|---|---|
| Gender | male | 49 | 90.40±9.41 | 8.73±1.25 | 2.05±0.31 | 49.15±8.14 |
| female | 40 | 89.04±8.67 | 8.83±1.15 | 2.14±0.36 | 50.21±7.26 | |
| Tvalue | 0.701 | 0.404 | 1.179 | 0.636 | ||
| Pvalue | 0.485 | 0.688 | 0.242 | 0.527 | ||
| Age | <65 | 51 | 88.96±9.32 | 8.82±1.20 | 2.10±0.31 | 49.00±7.82 |
| ≥65 | 38 | 90.89±8.71 | 8.71±1.23 | 2.08±0.36 | 50.47±7.64 | |
| Tvalue | 0.994 | 0.404 | 0.111 | 0.886 | ||
| Pvalue | 0.323 | 0.687 | 0.912 | 0.378 | ||
| Clinical stages | I | 32 | 85.21±6.97 | 8.02±0.88 | 1.88±0.20 | 43.57±4.68 |
| II | 36 | 89.92±8.41* | 8.73±0.87* | 2.03±0.20* | 50.01±4.68* | |
| III | 21 | 96.52±9.02*# | 10.00±1.17*# | 2.53±0.28*# | 58.20±7.39*# | |
| Fvalue | 12.444 | 27.678 | 56.223 | 46.179 | ||
| Pvalue | <0.001 | <0.001 | <0.001 | <0.001 | ||
| Lymphatic> metastasis | transferred | 31 | 97.57±8.08 | 9.51±1.27 | 2.34±0.36 | 56.18±7.26 |
| Not> transferred | 58 | 85.63±6.47 | 8.38±0.97 | 1.96±0.22 | 46.12±5.35 | |
| Tvalue | 7.594 | 4.727 | 5.312 | 6.792 | ||
| Pvalue | <0.001 | <0.001 | <0.001 | <0.001 |
Note: Compared with stage II, * P < 0.05 ; compared with stage III, # P < 0.05.
Differential analysis, functional enrichment analysis and pathway enrichment analysis: A total of 123 LC samples in TCGA were differentially analyzed and 1524 common DEGs were obtained, of which 566 were up-regulated and 958 were down-regulated (Supplemental Data Set1). The difference analysis results were visualized through a volcano plot (Figure 2A). The gene ontology enrichment analysis results showed that the biological functions are mainly production of molecular mediator of immune response, immunoglobulin production and hummoral immune response. The cellular components are mainly immunoglobulin complex, plasma membrane signaling receptor complex and T cell receptor complex. The molecular functions are mainly antigen binding, receptor ligand activity and signaling receptor activator activity (Figure 2B). The GSEA enrichment results are mainly MYOGENESIS, G2M_CHECKPOINT, UNFOLDED_PROTEIN_RESPONSE, MYC_TARGETS_V1, E2F_TARGETS and MTORC1_SIGNALING (Figure 2C).
Independent prognostic ability of groups: For evaluating the independent prognostic ability of the obtained gene classifier signatures, the clinically common factors like Grade, Age, TNM stage, gender and HSP90AA1 were registered as factor for analysis. A nomogram involving five items in LC was constructed, which is used as a clinically relevant quantitative method for predicting the mortality of LC patients. Obviously, we found that by adding points for each prognostic parameter, each patient will be assigned a total score value and higher total scores corresponded to poorer patient outcomes (Figure 3A). Timedependent C-index curves of different variables based on TCGA cohorts show the optimum performance of nomogram compared with other single factors (Figure 3B). Evaluate the prediction accuracy of HSP90AA1 on patient prognosis and survival through ROC curve (Figure 3C). Moreover, calibration plots for the TCGA LC reveal a similar performance of the nomogram to the developed prognostic model (Figure 3D-F).
Clinical indicator detection: There was no statistically significant difference in the proportions of gender, age, body mass index, smoking history, and drinking history among the three groups (P>0.05, Table 1). The plasma Hsp90a, CEA, SCC-Ag, and CA199 levels in the laryngeal cancer group were higher than those in the laryngeal vocal cord benign tumor group and the normal control group. The plasma Hsp90a, CEA, SCC-Ag, and CA199 levels in the laryngeal vocal cord benign tumor group were also higher than those in the normal control group. , the differences are statistically significant (P< 0.05, Table 2). There was no statistically significant difference in plasma Hsp90a, CEA, SCC-Ag, and CA199 levels among laryngeal cancer patients of different genders and ages (P>0.05); as the clinical stage of laryngeal cancer patients increased, their plasma Hsp90a, CEA, SCC-Ag, and CA199 levels increased Increased (P< 0.05); the plasma levels of Hsp90a, CEA, SCC-Ag, and CA199 in patients with lymph node metastasis were higher than those in those without lymph node metastasis (P< 0.05, Table 3).
Discussion
Laryngeal cancer is the most common malignant tumor of the head and neck. Despite improvements in treatment technology, some patients still relapse after treatment. Therefore, it is of great significance to find appropriate and effective prognostic indicators for laryngeal cancer [18]. In the era of, continued research on the function and regulation of the HSP90AA1 gene should be beneficial [19]. Studying expression profiling may also help to better understand the biology of HSP90AA1.
We used differential expression analysis to obtain the differential genes between the HSP90AA1 high expression group and low expression group, and obtained the key biological pathways and biological processes through functional enrichment analysis. Furthermore, based on clinical data, we analyzed the correlation between various indicators and HSP90a [20].
Heat shock protein 90 (HSP90) is an ATP-dependent molecular chaperone that forms a dynamic chaperone complex with HSP70 and co-chaperones, regulating the folding and stability of more than 200 client proteins, including AR. Cancer cells rely on HSP90 to maintain the stability and function of oncoproteins and buffer cellular stress caused by malignant transformation [21]. In tumor cells, HSP90 positively regulates the stability and activity of AR, and HSP90 inhibitors induce AR degradation and apoptosis [22]. Therefore, targeting HSP90 may provide a beneficial therapeutic strategy for the treatment of androgendependent tumor and androgen-independent [23].
We need to collect additional data sets for further analysis to validate our findings and further investigate the biological functions of these key genes. Second, more basic experiments are needed to verify the mechanisms by which key tumor genes and immune cells promote or inhibit tumor cell growth. In the future, more functional studies are needed to better characterize the roles of key genes and immune cells in LC. We strongly recommend further research on this topic to gradually increase the scholarly impact of these genetic biological evidences.
Declarations
Consent for publication: All authors approved the publication of the article.
Authors’ contributions: JW designed the study, performed the major data analysis, and drafted the manuscript. HC, PX provided funding source, designed, oversaw, and supervised the project and edited, reviewed, and finalized the paper. All the authors were involved in experimental studies. All authors contributed to the article and approved the submitted version.
Supplemental digital content: Results of differential expression analysis of HSP90AA1 between high and low expression groups.
References
- Law AB, Schmitt NC. Laryngeal Anatomy, Molecular Biology, Cause, and Risk Factors for Laryngeal Cancer. Otolaryngol. Clin. North Am. 2023; 56: 197-203.
- Leblanc A, Thomas TV, Bouganim N. Chemoradiation for Locoregionally Advanced Laryngeal Cancer. Otolaryngol. Clin. North Am. 2023; 56: 285-293.
- Cui J, et al. Cancer germline antigen gene MAGEB2 promotes cell invasion and correlates with immune microenvironment and immunotherapeutic efficiency in laryngeal cancer. Clin. Immunol. Orlando Fla. 2022; 240: 109045.
- Hoter A, El-Sabban ME, Naim HY. The HSP90 Family: Structure, Regulation, Function, and Implications in Health and Disease. Int. J. Mol. 2018; 19: 2560.
- Solárová Z, Mojžiš J, Solár P. Hsp90 inhibitor as a sensitizer of cancer cells to different therapies (review). Int. J. Oncol. 2015; 46: 907-926.
- Li G, et al. Berberine regulates the Notch1/PTEN/PI3K/AKT/ mTOR pathway and acts synergistically with 17-AAG and SAHA in SW480 colon cancer cells. Pharm. Biol. 2021; 59: 21-30.
- Sperandio FF, et al. Low-level laser therapy can produce increased aggressiveness of dysplastic and oral cancer cell lines by modulation of Akt/mTOR signaling pathway. J. Biophotonics. 2013; 6: 839-847.
- Mellatyar H, et al. Targeted cancer therapy through 17-DMAG as an Hsp90 inhibitor: Overview and current state of the art. Biomed. Pharmacother. Biomedecine Pharmacother. 2018; 102: 608-617.
- Tomczak K, Czerwińska P, Wiznerowicz M. The Cancer Genome Atlas (TCGA): An immeasurable source of knowledge. Contemp. Oncol. Poznan Pol. 2015; 19: 68-77.
- Han X, et al. Identification of immunocell infiltrates and effective diagnostic biomarkers in laryngeal carcinoma. Medicine (Baltimore). 2023; 102: 32548.
- Ding R, et al. Identification of Breast Cancer Subtypes by Integrating Genomic Analysis with the Immune Microenvironment. ACS Omega. 2023; 8: 12217-12231.
- Yang W, et al. BTG2 and SerpinB5, a novel gene pair to evaluate the prognosis of lung adenocarcinoma. Front. Immunol. 2023; 14: 1098700.
- Identification of cytokine‑predominant immunosuppressive class.pdf.
- Ding R, et al. Identification of immunosuppressive signature subtypes and prognostic risk signatures in triple-negative breast cancer. Front. Oncol. 2023; 13: 1108472.
- Wang J, et al. Systematic investigation of the mechanism of herbal medicines for the treatment of prostate cancer. Aging. 2023. doi:10.18632/aging.204516.
- Li M, Ding R, Yang X, Ran D. Study on Biomarkers Related to the Treatment of Post-Stroke Depression and Alternative Medical Treatment Methods. Neuropsychiatr. Dis. 2022; 18: 1861-1873.
- Diez M, Serum CEA. CA125, and SCC antigens and tumor recurrence in resectable non-small cell lung cancer. Int. J. Biol. 1995; 10: 5-10.
- Boyle K, Jones S. Functional outcomes of early laryngeal cancer - endoscopic laser surgery versus external beam radiotherapy: A systematic review. J. Laryngol. 2022; 136: 898-908.
- Birbo B, Madu EE, Madu CO, Jain A, Lu Y. Role of HSP90 in Cancer. Int. J. Mol. 2021; 22: 10317.
- Yu S, et al. Targeting HSP90-HDAC6 Regulating Network Implicates Precision Treatment of Breast Cancer. Int. J. Biol. Sci. 2017; 13: 505-517.
- Isaacs JS. Hsp90 as a Chaperone of the Epigenome: Insights and Opportunities for Cancer Therapy. Adv. Cancer Res. 2016; 129: 107-140.
- Kaplan KB, Li R. A prescription for stress the role of Hsp90 in genome stability and cellular adaptation. Trends Cell Biol. 2012; 22: 576-583.
- Centenera MM, et al. Co-targeting AR and HSP90 suppresses prostate cancer cell growth and prevents resistance mechanisms. Endocr. Relat. 2015; 22: 805-818.