
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
ACE inhibitor induced small bowel angioedema
*Corresponding Author : Santosh Kale
Lowell General Hospital, 1 Hospital Dr, Lowell, MA 01852, USA.
Email: santoshrkale@gmail.com
Received : Apr 24, 2024
Accepted : May 14, 2024
Published : May 21, 2024
Archived : www.jcimcr.org
Copyright : © Kal S (2024).
Citation: Kale S. ACE inhibitor induced small bowel angioedema. J Clin Images Med Case Rep. 2024; 5(5): 3065.
Description
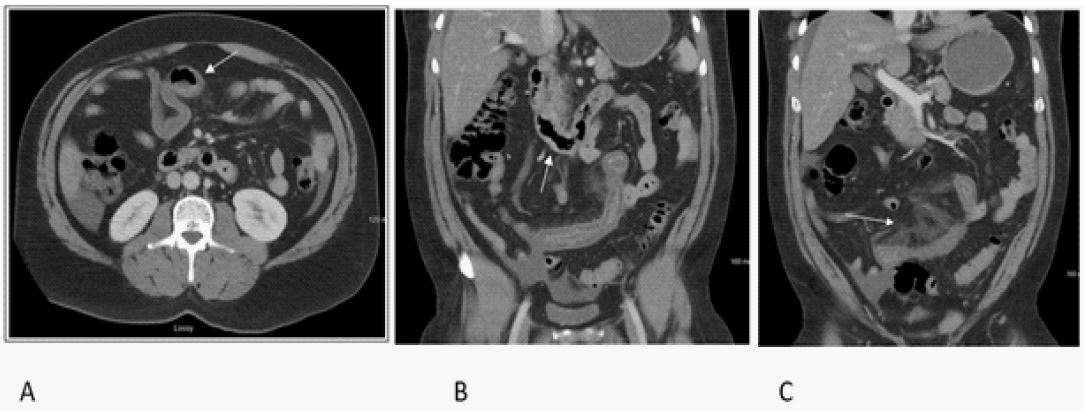
A 47 year old male with history of Hypertension presented to ER for abdominal pain. He visited his PCP 4 days ago, found to have hypertension and restarted on Lisinopril which patient had stopped taking since last 2 years. Since then he described gradual onset cramping pain near the epigastric region and denied any nausea, vomiting, diarrhea or constipation, also able to pass flatus. He denies any recent travel or prior history. He was afebrile and labs did not show any evidence of leukocytosis and lactate level was normal. CT abdomen with contrast showed edematous thickened small bowel wall (Figures 1A,1B) with associated mesenteric edema and vascular prominence with most severe involvement in mid abdominal loops (Figure 1C). He was switched from Lisinopril to Amlodipine for management of Hypertension. His symptoms gradually improved and diet was advanced. He tolerated regular diet on day 3 of hospitalization and discharged home with outpatient follow up.
ACE inhibitors have been widely used for management of blood pressure and cardiovascular benefits. Persistent cough, renal dysfunction, Hyperkalemia, anaphylaxis and rare cases of Angioedema are some of the notable side effects. ACE inhibitors work via blocking bradykinin degradation and increasing their level and this also thought to be mechanism of Angioedema [1]. Most cases happened soon after starting ACE Inhibitors but can also happen many years while on therapy and most commonly involve face, neck and lips and rarely involve the visceral organs [2]. There are no confirmatory laboratory test available making diagnosis difficult. Treatment often involves removal of the drug and supportive management as seen in our patient who had a dramatic recovery within 48-72 hrs once ACE inhibitors were stopped. Thus ACE inhibitor induced small bowel Angioedema is a rare presentation and delayed diagnosis can lead to significant morbidity for the patients [3].
References
- Alderman CP. Adverse effects of the angiotensin-converting enzyme inhibitors. Ann Pharmacother. 1996; 30(1): 55-61. doi: 10.1177/106002809603000110. PMID: 8773167.
- Taddei S, Bortolotto L. Unraveling the Pivotal Role of Bradykinin in ACE Inhibitor Activity. Am J Cardiovasc Drugs. 2016; 16(5): 309-21. doi: 10.1007/s40256-016-0173-4. PMID: 27260014.
- Quickfall D, Jakubovic B, Zipursky JS. Angiotensin-converting-enzyme inhibitor-induced angioedema. CMAJ. 2021; 193(20): 735. doi: 10.1503/cmaj.202308. PMID: 34001550; PMCID: PMC8177945.