
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Pathological complete response after 2 cycles of neoadjuvant chemotherapy combined with tislelizumab for stage III non-small cell lung cancer: A case report
Longfei Hu; Yuxin Huang; Ju Zhang*
The First Affiliated Hospital of Chongqing Medical University, China.
*Corresponding Author : Ju Zhang
The First Affiliated Hospital of Chongqing Medical University, China.
Tel: +86-15286162098.
Email: Zhangjucq@163.com
Received : Apr 25, 2024
Accepted : May 15, 2024
Published : May 22, 2024
Archived : www.jcimcr.org
Copyright : © Ju Z (2024).
Abstract
Introduction: The incidence of lung cancer is high, but the survival rate is low. For operable stage III non-small cell lung cancer, neoadjuvant chemotherapy, chemoradiotherapy or chemotherapy combined with immunotherapy, or postoperative adjuvant therapy can be used. We present neoadjuvant immunotherapy combined with chemotherapy for stage III lung cancer.
Case presentation: We report a case of stage IIIA lung squamous cell carcinoma treated with two cycles of tislelizumab combined with paclitaxel and nedaplatin. This patient had high Programmed death ligand 1(PD-L1) expression with Tumor Proportion Score (TPS) equal to 50%. Surgery was performed three weeks later, and postoperative pathology showed pathological complete response. Two cycles of tislelizumab combined with platinum-based chemotherapy were given after surgery, including one cycle of chemotherapy alone due to economic reasons. Currently, immunotherapy is being maintained.
Conclusion: Our study shows that tislelizumab plus platinum-based neoadjuvant therapy provides
Keywords: Non-small cell lung cancer; Neoadjuvant therapy; Tislelizumab; Case report.
Citation: Longfei H, Yuxin H, Ju Z. Pathological complete response after 2 cycles of neoadjuvant chemotherapy combined with tislelizumab for stage III non-small cell lung cancer: A case report. J Clin Images Med Case Rep. 2024; 5(5): 3066
Introduction
The most recent statistical report indicates that the five-year survival rate for lung cancer stands at a mere 25%. About 20% of Non-Small-Cell Lung Cancers (NSCLC) are stage III at initial diagnosis [1]. Neoadjuvant or adjuvant chemotherapy alone, combined with immune or targeted therapy are widely used in NSCLC [2]. Here, we present a special pathology of a patient with stage IIIA (T4N0M0) (American Joint Committee on Cancer eighth edition criteria) lung squamous cell carcinoma who underwent surgery after two cycles of platinum-based chemotherapy combined with tislelizumab, and the postoperative pathology indicated a pathological Complete Response (pCR). A pCR meant that 0% viable tumor cells were identified in the resected lung and lymph nodes.
Case presentation
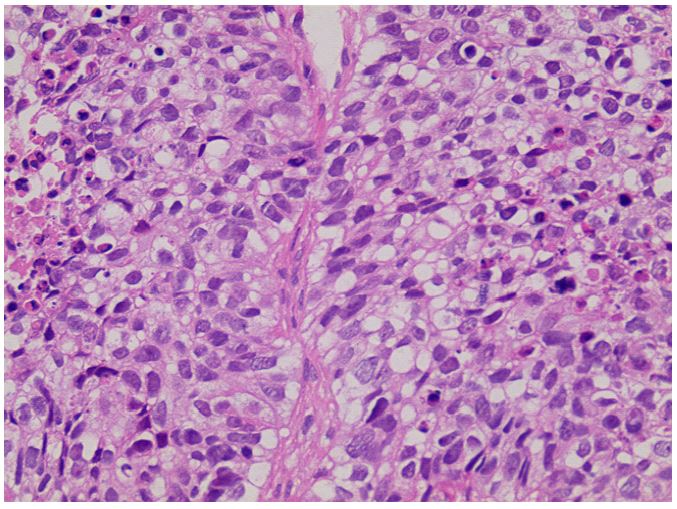
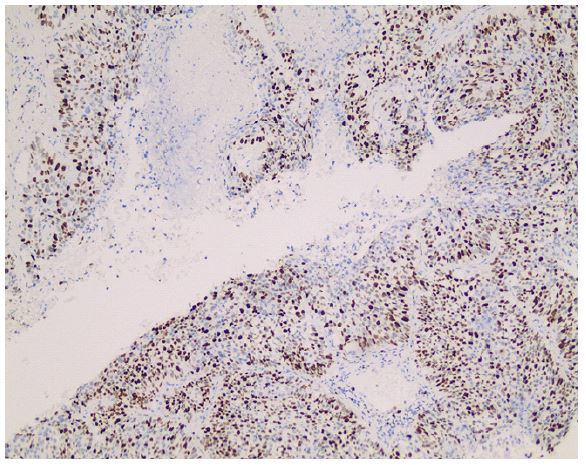
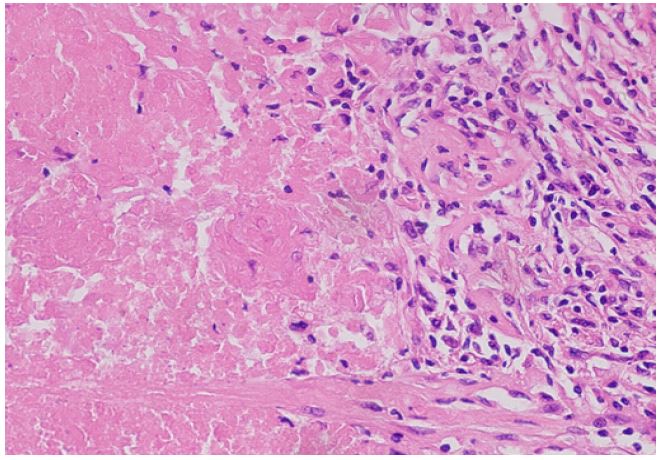
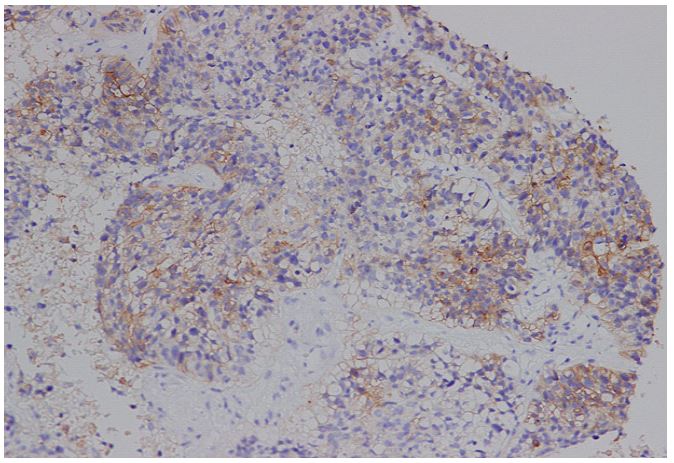
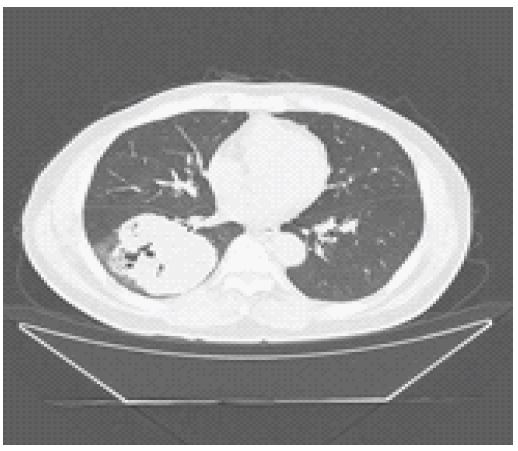
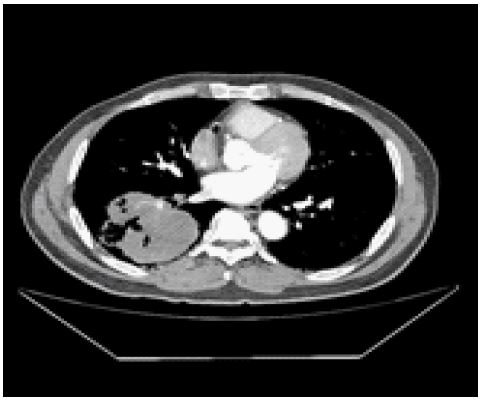
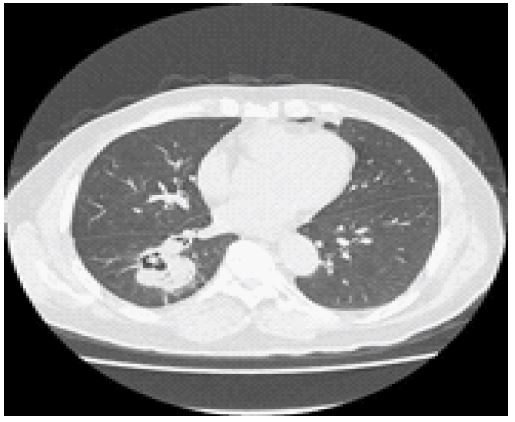
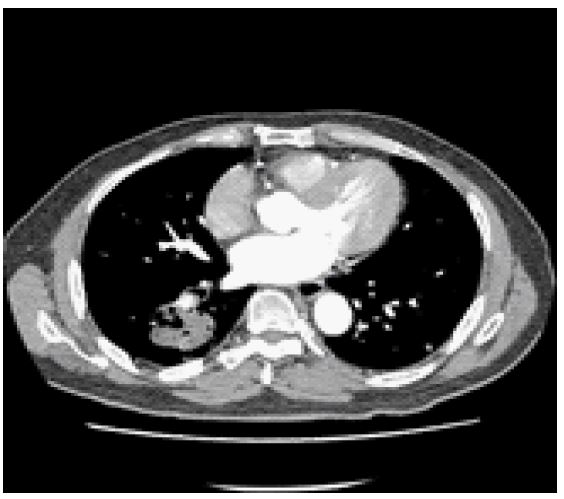
The patient, a 65-year-old male, presented with a persistent cough lasting for two months. A biopsy of the right lower lobe revealed squamous cell carcinoma with a Ki-67 (80%) expression (Figure 1). Programmed death ligand 1(PD-L1) assay expression was high, and Tumor Proportion Score (TPS) was equal to 50% (Figure 4). Computed Tomography (CT) examination showed a mass size of 9.1 x 8.2 cm in the lower lobe of the right lung (Figure 5b). The clinical stage was evaluated as T4N0M0, stage IIIA. Paclitaxel 240 mg on day 1 (135 mg/m2) combined with nedaplatin 80 mg on day 2 and 70 mg on day 3 (80 mg/m2) combined with tislelizumab 200 mg (day 1) were given for 2 cycles, 21 days for each cycle. Three weeks after the end of the second cycle of treatment, there was no obvious distant metastasis. Reexamination of CT showed that the size of the lung mass was 6.4 x 4.6 cm (Figures 7,8), which was smaller than that before treatment. Postoperative pathology showed a large amount of coagulative necrosis, combined with immunohistochemistry (epithelial marker CK was diffused positive), which was consistent with cancer necrosis, and no cancer residue was found (Figure 3). Lymph node examination showed no cancer metastasis. Postoperative chemotherapy combined with tislelizumab as adjuvant therapy for 2 cycles, and tislelizumab 200 mg as maintenance therapy.
Discussion
The prevalence of lung cancer is high, with NSCLC accounting for approximately 85% of all lung neoplasms, among which Squamous Cell Carcinoma (SCC) represents about 24% of NSCLC [3,4]. Surgical resection remains the primary treatment modal-ity for resectable NSCLC, but the risk of recurrence or metastasis is high after surgical resection alone [5]. A large number of studies have shown that NSCLC can benefit from neoadjuvant or adjuvant therapy, which is particularly important for its treatment [6,11]. For neoadjuvant therapy, most of them take three cycles of neoadjuvant chemotherapy, chemotherapy combined with immune, or chemotherapy combined with targeted therapy. The patient, however, only underwent two cycles of chemotherapy in conjunction with immunization, while the primary tumor exhibited a substantial size of approximately 9.1 x 8.2 cm. About three weeks after the end of the second cycle, the comprehensive evaluation showed that the tumor size was reduced to 6.4 x 4.6 cm, and then surgical treatment was performed, and the pathological results of the surgical specimen suggested pathological complete response. In a study by Wakelee et al. (KEYNOTE-671), patients with II, IIIA, or IIIB NSCLC who received four cycles of pembrolizumab plus chemotherapy followed by surgery had a pCR of 18.1%, as compared with 4.0% with placebo plus chemotherapy [12]. In the study by Lu et al. (Neotorch trail), in resectable NSCLC stage II-III, three cycles of neoadjuvant therapy with toripalimab plus chemotherapy resulted in a pCR of 24.8% versus 1.0% in the placebo-chemotherapy group [13]. In addition, studies of atezolizumab (IMpower 010) [14], Nivolumab (NADIM II) (CheckMate 816) [6,10], durvalumab (SAKK 16/14) [15] and others were not listed. Overall, three - or four-cycle neoadjuvant combination therapy followed by surgery improved pathological complete response by approximately 20% in patients with resectable NSCLC (stage II to III).
One retrospective study has demonstrated that the combination of neoadjuvant tislelizumab and chemotherapy yields a significant improvement in the pCR, with a reported rate of 34.78%. However, it should be noted that the sample size was limited to only 40 patients [16]. In the ongoing RATIONAL-315 (NCT04379635) trial, tislelizumab combined with platinum-based neoadjuvant therapy achieved a pCR of 40.7% (95% Confidence Interval [CI] 34.2-47.4) after three to four cycles, breaking the previous record of about 20% in immunotherapy plus chemotherapy. The rate of pCR was only 5.7% (95% CI 3.1-9.6) in the neoadjuvant chemotherapy group [17]. In our patient, a reduction of approximately 30% in the lung mass with neoadjuvant therapy and a postoperative pCR support these two studies, except that we used only two cycles of tislelizumab plus platinum-based neoadjuvant therapy. Some studies have shown that patients with high PD-L1 expression benefit from chemotherapy combined with immunity [6,12]. Ki-67 is an important indicator of tumor cell proliferation [18]. In our patient, both Ki-67 (80%) and PD-L1 (50%) were highly expressed, which may be related to the good prognosis of this patient. This patient is still receiving maintenance tislelizumab immunization, and long-term survival results are not available. However, it is not difficult to conclude from studies such as KEYNOTE-671 and CheckMate 816 that patients with pCR have better event-free survival [6,12].
Conclusion
In conclusion, tislelizumab combined with chemotherapy is beneficial as neoadjuvant treatment for stage III lung squamous cell carcinoma with high PD-L1 expression, and its long-term survival needs further follow-up. Further prospective studies are worth exploring.
Declarations
Author contributions: Conceptualization, Longfei Hu. and Ju Zhang; validation, Longfei Hu., Yuxin Huang., and Ju Zhang; formal analysis, Longfei Hu; investigation, Longfei Hu.,Yuxin Huang.; data curation, Longfei Hu.; writing—original draft prepa-ration, Longfei Hu.,Yuxin Huang. writing—review and editing, Longfei Hu., Ju Zhang; visualization, Yuxin Huang., and Ju Zhang.; supervision, Longfei Hu, Yuxin Huang, and Ju Zhang; project administration, Ju Zhang; All authors have read and agreed to the published version of the manuscript.”
Funding: This research received no external funding.
Institutional review board statement: The study was conducted in accordance with the Declaration of Helsinki, and approved by the Clinical Research Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (protocol code K2024-090-01, Ratification 13 March 2024).
Informed consent statement: Informed consent was obtained from all subjects involved in the study.Written informed consent has been obtained from the patient to publish this paper.
Data availability statement: Relevant data have been provided in the text, contact the corresponding author in case of doubt.
Acknowledgments: We thank the pathology department, molecular laboratory center, and Imaging Department for providing relevant images.
Conflicts of interest: The authors declare no conflicts of interest.
References
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024; 74: 12-49.
- Chaft JE, Shyr Y, Sepesi B, Forde PM. Preoperative and Postoperative Systemic Therapy for Operable Non-Small-Cell Lung Cancer. J Clin Oncol. 2022; 40: 546-55.
- Duma N, Santana-Davila R, Molina JR. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin Proc. 2019; 94: 1623-40.
- Takamochi K, Ohmiya H, Itoh M, Mogushi K, Saito T, Hara K, et al. Novel biomarkers that assist in accurate discrimination of squamous cell carcinoma from adenocarcinoma of the lung. BMC Cancer. 2016; 16: 760.
- Potter AL, Costantino CL, Suliman RA, Haridas CS, Senthil P, Kumar A, et al. Recurrence After Complete Resection for Non-Small Cell Lung Cancer in the National Lung Screening Trial. Ann Thorac Surg. 2023; 116: 684-92.
- Forde PM, Spicer J, Lu S, Provencio M, Mitsudomi T, Awad MM, et al. Neoadjuvant Nivolumab plus Chemotherapy in Resec-table Lung Cancer. N Engl J Med. 2022; 386: 1973-85.
- Herbst RS, Wu YL, John T, Grohe C, Majem M, Wang J, et al. Adjuvant Osimertinib for Resected EGFR-Mutated Stage IB-IIIA Non-Small-Cell Lung Cancer: Updated Results From the Phase III Randomized ADAURA Trial. J Clin Oncol. 2023; 41: 1830-40.
- Hui Z, Men Y, Hu C, Kang J, Sun X, Bi N, et al. Effect of Postoperative Radiotherapy for Patients With pIIIA-N2 Non-Small Cell Lung Cancer After Complete Resection and Adjuvant Chemotherapy: The Phase 3 PORT-C Randomized Clinical Trial. JAMA Oncol. 2021; 7: 1178-85.
- O’Brien M, Paz-Ares L, Marreaud S, Dafni U, Oselin K, Havel L, et al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB-IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): an interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol. 2022; 23: 1274-86.
- Provencio M, Nadal E, González-Larriba JL, Martínez-Martí A, Bernabé R, Bosch-Barrera J, et al. Perioperative Nivolumab and Chemotherapy in Stage III Non-Small-Cell Lung Cancer. N Engl J Med. 2023; 389: 504-13.
- Provencio M, Nadal E, Insa A, García-Campelo MR, Casal-Rubio J, Dómine M, et al. Neoadjuvant chemotherapy and nivolumab in resectable non-small-cell lung cancer (NADIM): an open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol. 2020; 21: 1413-22.
- Wakelee H, Liberman M, Kato T, Tsuboi M, Lee SH, Gao S, et al. Perioperative Pembrolizumab for Early-Stage Non-Small-Cell Lung Cancer. N Engl J Med. 2023; 389: 491-503.
- Lu S, Zhang W, Wu L, Wang W, Zhang P, Fang W, et al. Perioperative Toripalimab Plus Chemotherapy for Patients with Re-sectable Non-Small Cell Lung Cancer: The Neotorch Randomized Clinical Trial. Jama. 2024; 331: 201-11.
- Felip E, Altorki N, Zhou C, Csőszi T, Vynnychenko I, Goloborodko O, et al. Adjuvant atezolizumab after adjuvant chemo-therapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet. 2021; 398: 1344-57.
- Rothschild SI, Zippelius A, Eboulet EI, Savic Prince S, Betticher D, Bettini A, et al. SAKK 16/14: Durvalumab in Addition to Neoadjuvant Chemotherapy in Patients with Stage IIIA(N2) Non-Small-Cell Lung Cancer-A Multicenter Single-Arm Phase II Trial. J Clin Oncol. 2021; 39: 2872-80.
- Huang X, Zhu L, Liu J, Wang Y, Yu L, Wu S, et al. Safety and efficacy of tislelizumab plus chemotherapy as preoperative treatment in potentially resectable locally advanced non-small-cell lung cancer patients. Interdiscip Cardiovasc Thorac Surg. 2024; 38.
- Yue D, Wang W, Liu H, Chen Q, Chen C, Zhang J, et al. LBA58 Pathological response to neoadjuvant tislelizumab (TIS) plus platinum-doublet (PtDb) chemotherapy (CT) in resectable stage II-IIIA NSCLC patients (pts) in the phase III (Ph3) RA-TIONALE-315 trial. Annals of Oncology. 2023; 34: 1299.
- Xu J, Liu P, Da J, Hao J, Peng W, Sun G. Prognostic value of Ki-67 in stage I non-small-cell lung cancer: A meta-analysis in-volving 1931 patients. Pathol Res Pract. 2019; 215: 855-60.