
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Traumatic cataracts: Focus on rosette-shaped cataracts
Tlemcani Younes*; Boujaada Anass; Robbana Lobna; Elmajdoubi Kamal; Abdallah El Hassan
Ophthalmology B Department, Faculty of Medicine, Mohammed V University Rabat, Morocco.
*Corresponding Author : Tlemcani Younes
Ophthalmology B Department, Faculty of Medicine, Mohammed V University Rabat, Morocco.
Email: Yns.tlemcani@gmail.com
Received : Apr 25, 2024
Accepted : May 15, 2024
Published : May 22, 2024
Archived : www.jcimcr.org
Copyright : © Younes T (2024).
Abstract
Traumatic cataract is a serious and common condition that mainly affects young adults and children. We report the case of a 25-year-old female patient who presented for consultation with blurred vision that had been progressively developing for over a year and in whom the clinical examination revealed a rosette-shaped cataract.
Keywords: Subcapsular cataract; Trauma; Rosette cataract.
Citation: Younes T, Anass B, Lobna R, Kamal E, Hassan AE. Traumatic cataracts: Focus on rosette-shaped cataracts. J Clin Images Med Case Rep. 2024; 5(5): 3067.
Background
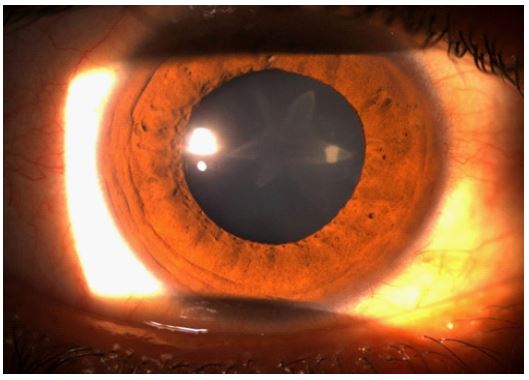
We report the case of a 25-year-old patient who presented for consultation with a visual blur that had been progressively developing for 1 year. The history found that the patient had suffered eye trauma from a punch more than 4 years previously. Ophthalmological examination revealed visual acuity of 7/10ths on the right and 10/10ths on the left. Slit-lamp examination revealed a posterior subcapsular cataract with thin blades forming a rose shape in the right eye (Figures 1 and 2); Examination of the dilated fundus revealed no abnormalities. B-scan ultrasonography showed a clear vitreous cavity without structural globe anomalies. Examination of the left eye was strictly normal. Intraocular pressure on the applanation tonometer was 13 mmHg in both eyes.

Discussion
Traumatic cataract is a serious and common condition that mainly affects young adults and children. It is caused by blunt or penetrating trauma, the mechanism most often incriminated is contrecoup, [4] which generates shock waves all along the path of the traumatic impact, leading to the formation of posterior subcapsular opacification in the form of a rosette or star and the prognosis depends on the associated anatomical lesions. As was the case for our patient [5]. The axial extension of these opacities can lead to a fast anteroposterior expansion, resulting in a rupture of the capsule, or even of the zonule in severe trauma. A complete ophthalmological examination is essential to detect any secondary lesions resulting from trauma, including wounds, hyphema, zonular rupture, lens dislocation, angle-recession glaucoma, phaco anaphylactic uveitis, retinal or choroidal detachment, optic neuropathy or retrobulbar hemorrhage. During surgery, it is important to handle the anterior capsule gently to minimize stress on the zonules, and phaco parameters should be decreased if zonular weakness is evident [5]. The functional prognosis of Traumatic cataracts depends mainly on the associated lesions, underlining the importance of a meticulous clinical examination [6]. In our patient’s case, since the visual acuity has been preserved, surgery is currently being deferred, with regular monitoring of the progress of her cataract.
Conclusion
The rosette-shaped cataract is a specific type of cataract where the lens appears to have a series of radial spoke-like opacities. In the case of our patient, where the surgery has been deferred, it’s important to closely monitor the progression of the rosette cataract. Regular follow-up examinations are crucial to assess any changes in visual acuity and their impact on daily life.
Acknowledgment: The authors declare that they have no conflicts of interest to this work.
References
- Fyodorov SN, Egorova EV, Zubareva LN. 1004 cases of traumatic cataract surgery with implantation of an intraocular lens. J Am Intraocul Implant Soc. 1981; 7(2): 147‑53.
- Sethi A, Ramasubramanian S. Double rosette cataract: A striking image! Indian J Ophthalmol. 2019; 67(1): 124‑5.
- Tasman w, Jaeger E. Traumatic cataract. Duane’s Clinical Ophthalmology. 1997; 13‑4.
- Shah MA, Shah SM, Shah SB, Patel CG, Patel UA. Morphology of traumatic cataract: does it play a role in final visual outcome? BMJ Open. 2011; 1(1): 000060.
- Singh RB, Thakur S, Ichhpujani P. Traumatic rosette cataract. BMJ Case Rep. 2018; 11(1): 227465.
- Okoye GS, Gurnani B. Traumatic Cataract. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. Disponible sur: http://www.ncbi.nlm.nih.gov/books/NBK594251/.