
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
New cases of dirofilariosis in Tunisia and literature review
Latifa Mtibaa1*; Souha Hannachi2; Rym Abid2; Fidaa Maatallah1; Riadh Battikh2; Boutheina Jemli1
1Laboratory of Parasitology, Military Hospital of Tunis, Tunisia.
2Department of Infectious Diseases, Military Hospital of Tunis, Tunisia.
*Corresponding Author : Latifa Mtibaa
Laboratory of Parasitology, Military Hospital of Tunis, Tunisia.
Email: mtibaalatifa@yahoo.frs
Received : Apr 27, 2024
Accepted : May 15, 2024
Published : May 22, 2024
Archived : www.jcimcr.org
Copyright : © Mtibaa L (2024).
Abstract
Dirofilariosis is a mosquito-borne zoonosis caused byfilarial nematodes of the genus Dirofilaria, subgenus Nochtiella. The definitive host is mainly the dog and the man constitutes a dead-end host. The most frequently detected parasitic species in humans is Dirofilaria repens responsible for the subcutaneous form of the infection with exceptional conjunctival migration. We report three new cases of human dirofilariasisin Tunisian elderly patients. The anamnesis revealed the presence of dogs in the entourage of all patients. The first had consulted for ocular redness not improved by eye drops. The ophthalmological examination showed a filiform nematode in the subconjunctival. The second and third cases were operated on for skin nodules on the forehead for one case and on the forearm for the other case. In all cases, parasitological and anatomopathological examinations allowed the identification of D. repens. Microfilariae were not detected in peripheral blood. Blood count and inflammatory markers were normal. The evolution was favorable without relapse in all cases. These cases remind us of the importance of thinking about dirofilariosis as a possible cause of infections in Tunisia, particularly in a suggestive clinical and epidemiological context.
Citation: Mtibaa L, Hannachi S, Abid R, Maatallah F, Battikh R, et al. New cases of dirofilariosis in Tunisia and literature review. J Clin Images Med Case Rep. 2024; 5(5): 3068.
Introduction
Dirofilariosis is an emerging mosquito-borne zoonosis with a worldwide distribution. It infects various domestic and wild animals naturally and canines are the principal reservoir hosts. Humans represent accidental hosts for these parasites as they usually do not develop to the fertile adult stage [1]. The prevalence of this disease seems to be increasing and new cases are being reported in South East, Central and Western Europe, Asia and Africa [2]. Although, it is challenging to define the prevalence of human dirofilariasis, considering the lack of a symptomatic disease and the absence of knowledge by physicians, leading to an underestimated number of clinical cases [1]. The dirofilarial life cycle consists of 5 stages that develop in a vertebrate host and in a mosquito vector (Aedes, Culex, Anopheles, Mansonia, and Amigeres) [1,3]. In humans, mosquitoes transmit the infective third-stage (L3) larvae during a blood meal that penetrate the host’s skin and the tissue reacts by trapping the developing larva in an inflammatory nodule [1]. Among nearly forty known species of Dirofilaria (D.) and at least five of them are known to cause accidental infections in humans reprensented mainly by D. repens and D. immitis [3]. In Tunisia, D. repens is the most prevalent species. Three main clinical forms are known depending on the site of infection: subcutaneous dirofilariasis (the most common), subconjunctival dirofilariasis and pulmonary dirofilariasis [4]. This paper has the goal to describe three new cases of human dirofilariosis due to D. repens in Tunisia, to update information about this infection in Tunisia.
Observations
Case 1: Subconjunctival dirofilariosis
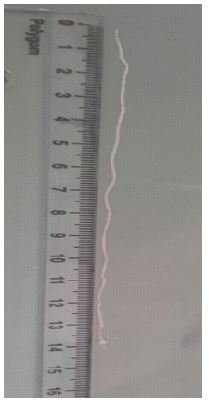
A 79-year-old man residing in the Cap Bon, with a history of hypertension and atrial fibrillation, working as a farmer with notion of contact with dogs. He complained of ocular redness in the right eye since 7 days for which symptomatic treatment with eye drops was prescribed. The evolution was marked by a non-improvement and a bilateralization of the ocular redness. Sedimentation rate was 32 mm (H1) and C-reactive protein was normal. The blood count was normal. The ophthalmological examination revealed a filiform nematode in the subconjunctival position, which was extracted (Figure 1) and sent to the laboratory of Parasitology of the military hospital of Tunis for identification. The specimen was 14 cm long (Figure 2). The direct microscopic examination of the wormidentified D. repens (Figure 3). The search for blood microfilariae after leucoconcentration was negative. No treatment was prescribed and the evolution was marked by a regression of ocular symptoms.
Case 2: Subcutaneous dirofilariosis
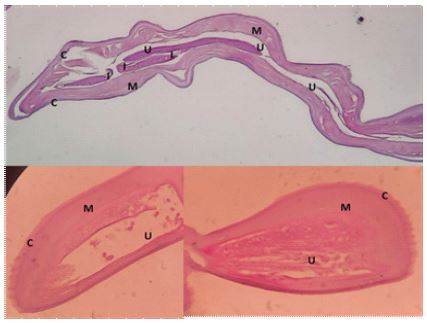
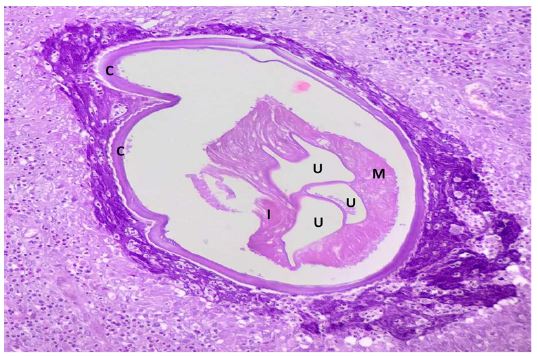
A 71-year-old man without underlying pathologies, residing in Tunis and having not traveled outside the country. He consulted for a painful swelling of the frontal region of the face associated with a right periorbital nodule which had evolved for 20 days without fever. The patient had revealed the notion of mosquito bites a month earlier. On physical examination, there was a periorbital skin nodule and a frontal swelling 3 and 4 cm in diameter, firm, fixed and painless (Figure 4). The blood count was normal. Sedimentation rate and C-reactive protein were normal. A facial CT scan showed a 25 mm right subcutaneous lesion, hypodense peripherally enhanced, and centrally liquefied, with thickening of the right periorbital soft tissues, without any bone lesion and without extension to the intraorbital space. The ophthalmological examination was normal. A search for diurnal and nocturnal microfilaraemia was negative. Surgical excision of the skin nodule was performed. The histological study showed the presence of three transverse sections of a female filarial worm surrounded by an important polymorphic inflammatory infiltrate. Analysis of the histological sections of the worm allowed the identification of D.repens (Figures 5 and 6). Retrospectively, the interrogation revealed the presence of cats and dogs in the surroundings. The treatment of choice therefore consisted of complete surgical resection of the nodule and removal of the worm. There is no relapse three months after discharge.
Case 3: Subcutaneous dirofilariosis
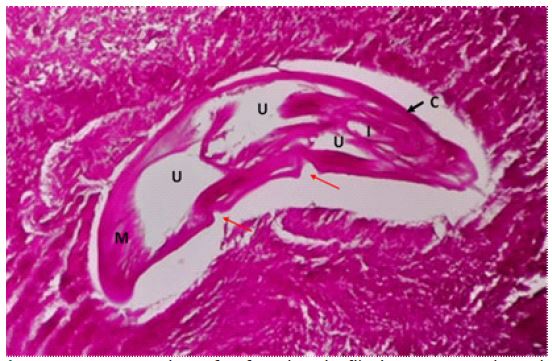
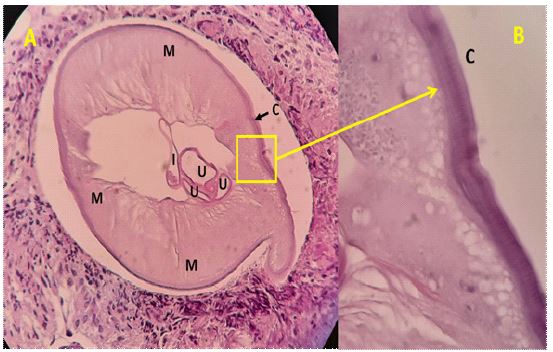
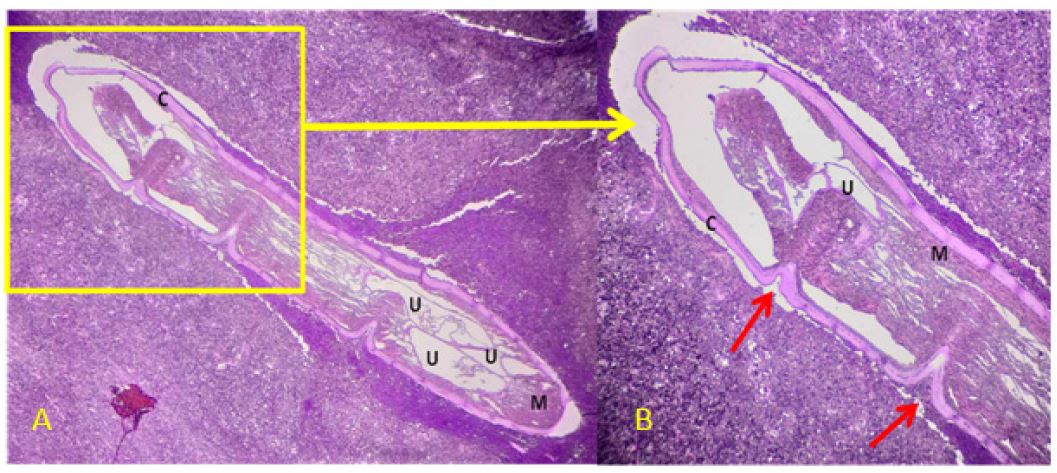
A 60-year-old man with a history of hypertension and dyslipidemia, residing in Tunis. The interrogation revealed contact with dogs. His history of illness dates back to 1 week after going out for a walk in the forest with the appearance of a painless skin swelling on the inner side of the forearm adjacent to a puncture lesion initially neglected by the patient. Faced with the increase in size of this lesion without associated signs of inflammation, he consulted a private practice surgeon who performed surgical excision of this mass. The macroscopic appearance reveals a subcutaneous fatty mass at the level of the multinodular forearm measuring 4 x 2 x 1 cm. The microscopic appearance shows abundant granulation tissue rich in neutrophils and eosinophils associated with the presence of transverse and longitudinal sections of a parasite compatible with a Dirofilaria. Hence, his transfer to the infectious diseases department. The physical examination was without abnormalities. Biology did not show hyperesinophilia and the search for microfilaremia was negative. A cardiac ultrasound and a thoraco-abdominopelvic scan requested were normal. Parasitological analysis of the sections allowed the identification of D.repens (Figures 7 and 8). No medical treatment was initiated with good progress.
Parasite description: The analysis of the parasites sections after HE and PAS staining allowed to visualize worms measuring between 300 and 600 μm in diameter, with a central digestive tract, three uterine cavities, a well-developed polymyary type muscular layer and a thick lamellar cuticle (20 μm) flaky and bumpy regularly and presenting serrations of 5 μm projecting outwards. This appearance was compatible with D. repens species (Figures 3,5-8).
Table 1: A review of Tunisian cases of human dirofilariasis.
| Author, year, reference | Age | Sex | Geographic origin | Location | Management | Species | Evolution |
|---|---|---|---|---|---|---|---|
| Kassar L. 1990[10] | 23 | M | Menzel Bourguiba | scrotal | Biopsy | - | Favorable |
| Chaabouni M.1990[25] | 55 | M | Kairouan | Conjonctival | - | - | - |
| Ben Said M. 1995[8] | 39 48 | FF | Gabes Sousse | Axillary Head | - | - | - |
| Mrad K.1999[26] | 32 | F | - | Mammary | Surgery | D.repens | - |
| Ayadi Kaddour A. 2003[27] | 23 21 | MM | Menzel Bourguiba | Scrotal Iliacfossa | - | - | - |
| Souissi A. 2004[23] | 27 | M | Bizerte | Scrotal | Surgery | D.repens | Favorable |
| Ziadi S. 2005[24] | 8 10 | MM | Kasserine Kairouan | Conjonctival Conjonctival | Surgery Surgery | D. immitis D.repens | Favorable Favorable |
| Hannachi Sassi S. 2006[28] | 21 | F | Tunis | Conjonctival | Surgery | D.repens | Favorable |
| Makni F. 2007[29] | 21 | F | Mahdia | Shoulder/thigh | Biopsy | D.repens | Favorable |
| Chaari C. 2008[11] | 19 21 | M F | Gabes Mahdia | Para-ombilical Shoulder/buttock | Surgery Biopsy | D.repens | Favorable Favorable |
| Kaouch E. 2010[30] | 40 | F | Cap-Bon | labial | Surgery | D.repens | Favorable |
| Saied W. 2011[31] | 4 | F | Tunis | Hand | Surgery | D.repens | Favorable |
| Ben Hassouna J. 2015[22] | 30 45 | FF | Ariana Nabeul | Mammary Mammary | Surgery Surgery | D.repens | Favorable Favorable |
| Idoudi S.2021[20] | 19 | F | East Central Tunisia | Lumbar | Surgery | D.repens | Favorable |
| El MatriK. 2020[21] | 60 | M | Tunis | Mammary | Surgery | D.repens | Favorable |
| Ourcases | 79 71 60 | MMM | CapBon Tunis Tunis | Conjonctival Frontal Forearm | Wormextraction Surgery Surgery | D.repens | Favorable Favorable Favorable |
M: Male; F: Female


Discussion
Human dirofilariasis is a disease rarely observed in humans and in Tunisia. We report here three cases diagnosed in Tunisians at the military hospital of Tunis. All patients lived in the north of Tunisia and didn’t travel outside Tunisia. They were all male with an average age of 70 years. Dirofilaria repens was identified in all cases. Contact with dogs was noted in all cases. Pollution, the ownership of cats and dogs, reservoirs of heartworm disease, as well as the facilitation of travel for these domestic animals may be factors that contribute to the emergence of the disease. Furthermore, global warming has increased transmission by mosquito vectors and the prevalence of canine microfilariae [5]. According to the literature, 5 species of Dirofilaria have been identified as the causative agent of reported cases in humans. The species most responsible is D. repens (72.22%) followed by D. immitis (6.94%), D. tenuis (1.04%), D. hongkongensis (0.87%) and D. ursi (0.17%) [6]. D. repens is distributed in Asia, Europe, Africa, mainly in the Mediterranean basin, while D. immitis is cosmopolitan [7-9]. In Tunisia, D. repens is the most prevalent species and 20 cases are published since the first case described in 1990 by Kassar et al. [10].
Clinically, D. repens manifests either as a wandering worm in the subcutaneous tissue, or as a dead worm forming a granulomatous nodule in the dermis or submucosa. These skin nodules generally develop over 6 months and are generally not painful [11]. They are erythematous, firm and elastic and primarily suggest a lipoma, a fibroma or an epidermal or sebaceous cyst [11]. Most cases of subcutaneous dirofilariasis were localized in the ocular region (74%) and in the upper limb region (11%) [12,13]. The clinical course can be severe, and symptoms may include vision impairment or even vision loss [12]. D. immitis most often causes pulmonary involvement in the human host as well as in the definitive host, but can also, more rarely, cause nodules in other tissues, mainly in the thoracic part [6,14,15]. L4 larvae can reach the small bronchi causing emboli with localized inflammation [16]. Pulmonary dirofilariasis causes nonspecific pulmonary signs, but it is often asymptomatic. Eosinophilia is associated. These pulmonary nodules can be mistaken for malignant nodules but the presence of larvae or adults of Diforilaria sp. histopathology surrounded by fibrosis and cellular infiltration with or without necrotic foci corrects the diagnosis [6,17].
The diagnosis of human heartworm disease is essentially based on the detection and identification of microfilariae in histology or adults in parasitology. Molecular and immunological techniques are used as complementary or alternative diagnostic methods [18]. Treatment of subcutaneous heartworm disease relies on excision of nodular granulomas in the lungs or subcutaneous tissue and careful extraction of adults. Each attempt should be designed to extract intact adult worms to avoid inflammatory reactions by antigen stimulation. No medical antihelminthic treatment is necessary [19]. In our first case, the extraction of the adult was successful. In the 2nd and 3rd cases, surgical removal of the skin nodule and the nematode was done. A good clinical evolution was noted in all cases.
Table 1 summarizes the different Tunisian cases of dirofilariosis published (n=20) with ours. Since 1990, 20 cases have been reported in Tunisia, eleven of which had a subcutaneous location (40%) [10,20]. Other cases have been reported with different locations (ocular (25%); breast (20%); scrotal (15%); labial (5%)) [20-23]. The average age of the patients was 27 years with extremes of 4 and 55 years. The Tunisian patients reported came from the north, center and south in 52.6% (10/19), 36.8% (7/19) and 10.5% (2/19), respectively. A female predominance was noted with a sex ratio of 0.8 (9/11). The diagnostic management was specified in 14 cases, eleven of which were by surgical excision and by biopsy in 3 cases. The species diagnosed was mainly D. repens (92.3%: 12/13). A single case of D. immitis has been reported with a conjunctival localization [24]. A good clinical outcome was reported in 14 cases. In the rest of the cases it was not specified.
Conclusion
Over the last decades, we have witnessed an increase in the prevalence of human dirofilariasis which may be underestimated due to its great clinical variability which can hamper its clinical and paraclinical diagnosis. These new cases in Tunisia remind us of the importance of thinking about dirofilariosis as a possible cause of infections in Tunisia, particularly in a favorable clinical and epidemiological context. Other studies should focus on human dirofilariasis in order to understand its true prevalence, detect endemic areas, establish less invasive diagnostic tools and improve its clinical management.
References
- Benzaquen M, Marmottant E, Parola P, Berbis P. La dirofilariose cutanée. Annales de Dermatologie et de Vénéréologie. 2017; 144: 607–11. https: //doi.org/10.1016/j.annder.2017.05.006.
- MIRON, Liviu,. Guide des principales maladies parasitaires transmises des animaux non-humains aux humains - La dirofilariose chez les humains et les animaux. 2016. 2016th ed. Université des Sciences Agricoles et de Médecine Vétérinaire (USAMV), Iasi (Roumanie); n.d.
- R V, C S, Sunil B, Kadwalia A, Bhoomika, P M, et al. Dirofilariasis: An emerging zoonoses. J Pharmacogn Phytochem. 2019; 8: 3014–8.
- Hennocq Q, Helary A, Debelmas A, Monsel G, Labat A, Bertolus C, et al. Oral migration of Dirofilaria repens after creeping dermatitis. Parasite n.d.; 27: 16. https: //doi.org/10.1051/parasite/2020015.
- Capelli G, Genchi C, Baneth G, Bourdeau P, Brianti E, Cardoso L, et al. Recent advances on Dirofilaria repens in dogs and humans in Europe. Parasites Vectors. 2018; 11: 663. https: //doi.org/10.1186/s13071-018-3205-x.
- Simón F, Diosdado A, Siles‐Lucas M, Kartashev V, González‐ Miguel J. Human dirofilariosis in the 21st century: A scoping review of clinical cases reported in the literature. Transbounding Emerging Dis. 2022; 69: 2424–39. https: //doi.org/10.1111/tbed.14210.
- Dantas-Torres F, Otranto D. Dirofilariosis in the Americas: a more virulent Dirofilaria immitis? Parasites & Vectors. 2013; 6: 288. https: //doi.org/10.1186/1756-3305-6-288.
- Said MB, Korbi S, Abdelhedi M, Sriha B, Khochtali H. La dirofilariose sous-cutan6e humaine : propos de deux nouveaux cas tunisiens n.d.
- Babay A, Hannachi S, Mtibaa L, Elleuch W, Jemli B, Battikh R. A new Tunisian case of subcutaneous dirofilariasis. 2022; 2.
- Kassar L, Kchir N, Boubaker S, Haouet S, Bouratbine A, Chatti S, et al. A case of subcutaneous dirofilariasis in Tunisia. . Bull Soc Pathol Exot. 1990; 83: 517–20.
- Châari C, Zouari I, Gouiâa N, Fakhfakh I, Ayadi L, Kallel R. Dirofilariose cutanée: à propos de deux cas tunisiens. Rev Tu Infectiol. 2008; 2: 25–7.
- Pampiglione S, Rivasi F. Human dirofilariasis due to Dirofilaria (Nochtiella) repens: an update of world literature from 1995 to 2000. Parassitologia. 2000; 42: 231–54.
- Centers for Disease Control and Prevention. Dirofilariasis En ligne. . Juil 2019Consulté le 12 déc 2023. . Consultable à l.’URL: https: //www.cdc.gov/dpdx/dirofilariasis/index.html
- Haro A, Tamiya S, Nagashima A. A rare case of human pulmonary dirofilariasis with a growing pulmonary nodule after migrating infiltration shadows, mimicking primary lung carcinoma. International Journal of Surgery Case Reports. 2016; 22: 8–11. https: //doi.org/10.1016/j.ijscr.2016.03.023.
- Palicelli A, Veggiani C, Rivasi F, Gustinelli A, Boldorini R. Human Pulmonary Dirofilariasis Due to Dirofilaria immitis: The First Italian Case Confirmed by Polymerase Chain Reaction Analysis, with a Systematic Literature Review. Life. 2022; 12: 1584. https: //doi.org/10.3390/life12101584.
- Simón F, Siles-Lucas M, Morchón R, González-Miguel J, Mellado I, Carretón E, et al. Human and Animal Dirofilariasis: the Emergence of a Zoonotic Mosaic. Clin Microbiol Rev. 2012; 25: 507–44. https: //doi.org/10.1128/CMR.00012-12.
- Fournier G, Morquin D, Goulabchand R, Tingaud C, De Boutray M. Dirofilariose autochtone intra-musculaire temporale. Médecine et Maladies Infectieuses. 2018; 48: 424–6. https: //doi.org/10.1016/j.medmal.2018.03.009.
- Benzaquen M, Marmottant E, Parola P, Berbis P. La dirofilariose cutanée. Annales de Dermatologie et de Vénéréologie. 2017; 144: 607–11. https: //doi.org/10.1016/j.annder.2017.05.006.
- Diaz JH. Increasing Risks of Human Dirofilariasis in Travelers. J Travel Med. 2015; 22: 116–23. https: //doi.org/10.1111/jtm.12174.
- Idoudi S, Youssef M, Soua Y, Achour A, Babba H, Zili J. Subcutaneous dirofilariasis in a Tunisian patient. IJDVL. 2021; 87: 390–2. https: //doi.org/10.25259/IJDVL_995_19.
- El Matri K, Falfoul Y, Elloumi A, Maamouri M, Chebil A, Matri M, et al. Human ocular dirofilariasis masquerading as a malignancy. Journal Français d’Ophtalmologie. 2020; 43: e365–8. https: //doi.org/10.1016/j.jfo.2020.02.025.
- Ben Hassouna J, Jbir I, Mezghani B, El Amine O, Zemni I, Mrad K, et al. Dirofilariasis of the breast: Two new cases in Tunisia. Médecine et Santé Tropicales. 2015; 25: 327–30. https: //doi.org/10.1684/mst.2015.0492.
- Dirofilariose sous-cutanée à Dirofilaria repens en Tunisie : Une observation à localisation scrotale | Semantic Scholar n.d. https: //www.semanticscholar.org/paper/Dirofilariose-sous-cutan%C3%A9e-%C3%A0-Dirofilaria-repens-en-Souissi-Klibi/70da54a7dbb03503795327745fe420dba6a742f5 (accessed January 13, 2024).
- Ziadi S, Trimeche M, Mestiri S, Mokni M, Trabelsi A, Ben Abdelkader A, et al. La dirofilariose sous-conjonctivale humaine: À propos de deux cas tunisiens. Journal Français d’Ophtalmologie. 2005; 28: 773.e1-773.e4. https://doi.org/10.1016/S0181-5512(05)80993-3.
- Chaabouni M, Sallami R, Ben Said M, Ben Rachid MS, Romdane K. Conjunctival dirofilariasis, a case discovered in the Kairouan region. . Arch Inst Pasteur Tunis. 1990; 67: 5–9.
- Mrad K, Romani-Ramah S, Driss M, Bougrine F, Hechiche M, Maalej M, et al. Mammary Dirofilariasis: A Case Report. Int J Surg Pathol. 1999; 7: 175–8. https: //doi.org/10.1177/106689699900700308.
- Ayadi-Kaddour A, Ouertani L, Bouraoui S, Zidi Y, Mekni A, Kchir N, et al. Human subcutaneous dirofilariasis: Two new cases in Tunisia. Nouvelles Dermatologiques. 2003; 22: 17–9.
- Hannachi Sassi S, Abid L, Dhouib R, Mrad K, Bouguila H, Abbes I, et al. Dirofilariose conjonctivale à Dirofilaria repens. À propos d′un nouveau cas tunisien. Journal Français d’Ophtalmologie. 2006; 29: 197.e1-197.e4. https://doi.org/10.1016/S0181-5512(06)73773-1.
- Makni F, Hachicha L, Abdelkafi N, Guiaâ N, Sellami H, Sellami T, et al. Dirofilariose sous-cutanée à Dirofilaria repens dans la région de Sfax (Tunisie). Annales de Dermatologie et de Vénéréologie. 2007; 134: 53-54. https://doi.org/10.1016/S0151-9638(07)88990-3.
- Kaouech E, Becheur M, Cheikh M, Belhadj S, Kallel K, Chaker E. Dirofilariose sous-cutanée en Tunisie : une observation à localisation labiale. Cahiers d’études et de Recherches Francophones / Santé. 2010; 20: 47–8. https://doi.org/10.1684/san.2009.0172.
- Saied W, Amara K, Bouchoucha S, Khaled S, Mrad K, Nessib MN, et al. Une étiologie inhabituelle de nodule de la main : la dirofilariose péritendineuse. Chirurgie de la Main. 2011; 30: 66–8. https: //doi.org/10.1016/j.main.2010.10.012.