
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Disseminated staphylococcal infection (involving bilateral sacroiliac joints and sternoclavicular joint) in a hemodialysis patient
Prem P Varma*; Prateek Kumar
Primus Hospital, New Delhi, India.
*Corresponding Author : Prem P Varma
Primus Hospital, New Delhi, India.
Email: varmapp123@rediffmail.com
Received : Apr 27, 2024
Accepted : May 16, 2024
Published : May 23, 2024
Archived : www.jcimcr.org
Copyright : © Varma PP (2024).
Abstract
Pyogenic sacroiliitis is a rare infection and has not been reported in a hemodialysis patient. We report a case of disseminated staphylococcal infection with bilateral sacroiliitis, sternoclavicular arthritis and right sternocleidomastoid abscess in a dialysis patient. Prompt diagnosis and institution of antibiotics resulted in complete recovery.
Citation: Varma PP, Kumar P. Disseminated staphylococcal infection (involving bilateral sacroiliac joints and sternoclavicular joint) in a hemodialysis patient. J Clin Images Med Case Rep. 2024; 5(5): 3069.
Case report
A 52 year old female, with end stage renal disease secondary to hypertensive kidney disease has been on regular haemodialysis for last 8 years. She presented in October 2021, with acute bilateral lower back and hip pain of 7-8 days duration. Pain was severe and radiating to both legs (Right>Left). She was not able to move her right leg and had been bed bound for 5 days. There was no preceding history of fever, urinary symptoms, loss of sensations in lower limbs, joint pain or trauma. Her bladder and bowel control was intact and there was no pain or weakness in upper limbs. There was history of small pustule developing near fistula puncture site a fortnight prior to present hospitalisation, which burst and healed over next week.
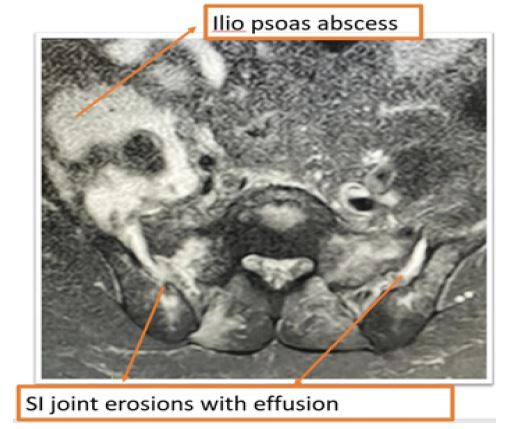
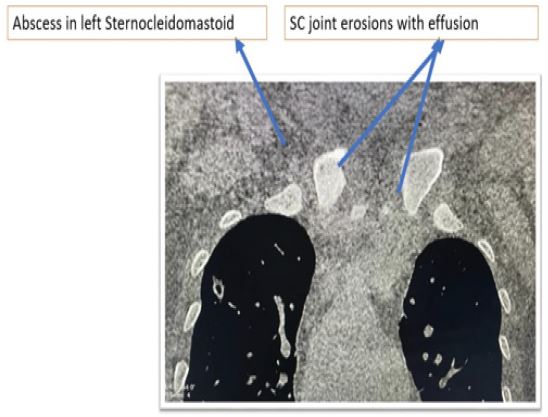
On presentation to ER she was awake and alert, afebrile, hypotensive with a blood pressure of 88/60 mm of Hg and pulse rate of 98 per min. Examination revealed tenderness over lower back, in the region of sacroiliac joints. There was no focal neurologic deficit but movements of lower limbs were restricted due to pain. Other systemic examination was unremarkable. Investigations revealed a ESR of 135 mm in first hour, haemoglobin of 11.4 gm/dl with total leucocyte count of 22,390/cmm. CRP was 70 mg/L and procalcitonin level was 24.3 ng/ml. Blood urea was 113 mg and creatinine 11.5 mg/dl. LFT showed serum bilirubin of 1.2 mg/dl, ALT/AST of 81/45 U/L. MRI pelvis showed asymmetric bilateral sacroiliac joint effusion (Rt>Lt) with irregular eroded articular margins, with pus tracking down from both joints with collections over right iliopsoas (6.5 x 5.5 cm) and left piriformis muscle (5 x 1 cm) (Figure 1). A diagnosis of tubercular cold abscess was considered in view of endemicity and absence of fever. A screening MRI of thoraco-lumbar spine to assess for source of iliopsoas abscess returned normal. Echocardiogram did not show any evidence of vegetations. USS guided diagnostic pus aspiration was done which showed gram positive cocci and culture grew staphylococcus aureus. AFB stain and Genexpert for tuberculosis was negative. Blood culture also grew Staphylococcus aureus. She was started on vancomycin, linezolid and analgesics. After a week of antibiotics, she started showing improvement. Pain subsided, leg mobility became near normal and leucocyte count came down to 11200/cmm; but she developed pain and swelling over left sternoclavicular joint. On examination, left sternoclavicular joint was found to be swollen and tender. CT neck and chest was done which showed bilateral sternoclavicular joint erosions with left sided collection. CT also detected right sternocleidomastoid muscle abscess of size 2.4x3 cm (Figure 2). About 10 ml pus was drained from sternocleidomastoid abscess and abscess near left sternoclavicular joint. This aspirate did not grow any bacteria and was negative for AFB and Gene expert. Whole body PET scan was done to assess for any additional foci, however it did not yield any other focus of bone or muscle infection.
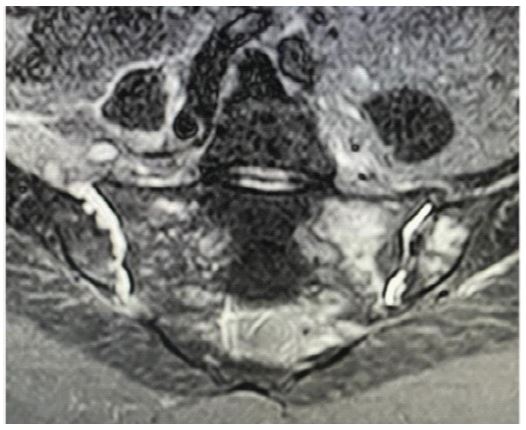
After 2 weeks of antibiotics, pain had regressed significantly and she started to sit up. Her leucocyte count was normal and procalcitonin was 5.7 ng/ml. After 4 weeks of antibiotics, she became ambulant, pain free, with marked improvement in swelling. A repeat MRI of pelvis showed regression of fluid collection in both SI joint although swelling around joints still persisted. Iliopsoas abscess was more organised and there was regression of pus collection over piriformis (Figure 3). The probable source of this disseminated musculoskeletal staphylococcal infection was the pustule which developed adjacent to AV fistula puncture site. A review in Dec 2022, found her doing well, with no backache.s
Discussion
Infectious Sacroiliitis (ISI) is a rare disease, accounting for 1-2% of all cases of septic arthritis. Poor vascularisation of SI joint makes it less prone for infection via hematogenous route and with aging vascularity becomes poorer, therefore ISI is common in younger population [1,2]. Most of the reported cases are among children or immunocompromised individuals, however in 30% cases precipitating factor may not be found. It usually gets diagnosed late because of non-specific symptoms [1,2]. In a French series of eight Rheumatology centres, 39 cases of ISI were seen over a 16 year period and only in 5 cases diagnosis could be made on admission. Majority of patients present with backache, buttock pain or gluteal pain with restriction of leg mobility. Fever and backache may be a feature in 70% of the patients. In two series comprising of 18 and 39 cases of ISI, mean time to arrive at diagnosis was 17.9 days and 43.3+69.1 days respectively [1,2]. Staphylococcus aureus is responsible for most cases of pyogenic sacroiliitis. In a Chinese series of 110 cases, 71 were due to staphylococcus infection, 24 were due to Mycobacterium tuberculosis and 15 due to Brucella [3]. In another series of 22 patients 8 were tubercular, 3 due to Brucella and rest 11 were pyogenic [4]. Rarely streptococcus and gram negative organisms e.g. pseudomonas, E coli are responsible organisms [5]. Radiography and CT scan are useful diagnostic modalities. However MRI is the modality of choice [2]. Besides infection, sacroiliac pain can also be caused by ankylosing spondylitis, osteoarthritis, tumours, sprain or fractures and these are the usual differentials [1-4]. In dialysis patients secondary hyperparathyroidism can also mimic sacroiliitis [6]. Literature search for ISI among dialysis population shows only a single case report in a peritoneal dialysis patient. Involvement in ISI has been invariably unilateral. In the largest series of 110 cases, all but 3 had unilateral involvement [3]. Isolation of offending organism requires pus aspiration from joint or abscess. If that is challenging, blood cultures can be helpful. Prolonged antibiotic course is the usual line of management with or without local pus drainage. Duration of therapy is unclear but most described cases in literature received antibiotics for 6-12 weeks with or without pus drainage. Initially parental antibiotics (for 2-4 weeks, till symptoms subside) and later oral antibiotics can be given [1-4]. Patients who develop instability of the joint, need arthrodesis to alleviate the pain [7]. In our case, patient developed bilateral sacroiliitis, left sternoclavicular arthritis (SCJ) and sternocleidomastoid muscle abscess over a period of 7-9 days. It is highly likely, that the infection had disseminated to these sites prior to presentation, though sacroiliac involvement was first to be identified. Our patient had bilateral sacroiliitis which has rarely been reported. It is possibly her immunocompromised state that led to disseminated disease. To the best of our knowledge this is the first case report of ISI in a haemodialysis patient. Prompt diagnosis and early initiation of antibiotics resulted in complete recovery. One should keep ISI in mind in a dialysis patient presenting with hip pain and restricted leg mobility.
References
- Matt M, Denes E, Weinbreck P. Infectious Sacroiliitis: Retrospective analysis of 18 case patients. Medicine et Maladies Infectieuses. 2018; 18: 333-388.
- Hermet M, Minichiello E, Flipo RM, Dubost JJ, Allanore Y et al. Infectious sacroiliitis: A retrospective, multicentre study of 39 adults. BMC Infect Dis. 2012; 12: 305.
- Wang G, Wang Y, Zhu J, Jin J, Zhao Z, Zhang J, Huang F. Analysis of clinical and imaging characteristics of infectious sacroiliac arthritis and review of literatures. Zhonghua Nei Ke Za Zhi. 2015; 54(5): 420-5.
- Wang YY, Zhao Z, Zhang JL, Huang F. Clinical and imaging characteristics of 110 patients with infectious sacroiliitis. Zhonghua Nei Ke Za Zhi. 2020; 59(2): 134-139.
- Tristano AG. Sacroiliac pain in a dialysis patient. BMJ Case Rep. 2009; 2009: bcr06. 2009.1934. doi:10.1136/bcr.06.2009.1934
- Kreutzinger, V., Diekhoff, T., Liefeldt, L. et al. Asymptomatic secondary hyperparathyroidism can mimic sacroiliitis on computed tomography. Sci Rep. 2021; 11: 4323. https://doi.org/10.1038/s41598-021-83989-1
- Passaplan C, Simonin A, Maestretti G, Gautier E. Management of Instability following Pyogenic Sacroiliitis: Technical Case Report. Case Rep Orthop. 2020; 2020: 3409306. Published 2020 Feb 29. doi:10.1155/2020/3409306
- Wafa Chebbi, Saida Jerbi, Wassia Kessomtini, Asma Fradi, Baha Zantour, Mohamed Habib Sfar, “Pyogenic Sacroiliitis and Pyomyositis in a Patient with Systemic Lupus Erythematous”, Case Reports in Rheumatology. 2014; 925961:4. 2014. https://doi.org/10.1155/2014/925961
- Kim S, Lee KL, Baek HL, Jang SJ, Moon SM, et al. (2013) A case of acute pyogenic sacroiliitis and bacteremia caused by community-acquired methicillin-resistant staphylococcus aureus. Infect Chemother 2013; 45: 441-445.
- Nogueira, Helder; Pereira, Joana; Couto, André; Alves, Jorge; Lopes, Daniel; Freitas, Joana; Alegrete, Nuno; Costa, Gilberto. Pyogenic Sacroiliitis in a Pediatric Patient: A Rare Case of Infection by Streptococcus intermedius, JAAOS: Global Research and Reviews: 2018; 2(7): e052 doi: 10.5435/JAAOSGlobal-D-17-00052