
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Chlamydia trachomatis: An unusual cause of rectosigmoiditis
Tsomidis I1; Kouroumalis E2*
1Evangelismos Private Hospital, 8021 Paphos, Cyprus.
2Department of Gastroenterology, PAGNI University Hospital, University of Crete School of Medicine, 71500 Heraklion, Crete, Greece.
*Corresponding Author : Kouroumalis E
Department of Gastroenterology, PAGNI University Hospital, University of Crete School of Medicine, 71500 Heraklion, Crete, Greece.
Tel: 00306944711386,
Email: kouroumi@uoc.gr
Received : Apr 29, 2024
Accepted : May 17, 2024
Published : May 24, 2024
Archived : www.jcimcr.org
Copyright : © Kouroumalis E (2024).
Abstract
Chlamydia trachomatis, is a frequent pathogen causing sexually transmitted proctitis. We report a case of a man with chlamydia-related recto-sigmoiditis without a history of having sex with other men or multiple sexual partners who was HIV negative. The colonoscopy showed multiple discrete aphthous ulcers of the rectum and sigmoid colon with inflammation and mucosal friability. Initial histology was interpreted as Inflammatory Bowel Disease (IBD). Treatment failure raised the possibility of non-IBD inflammation and serology confirmed chlamydia trachomatis procto-sigmoiditis. Treatment with doxycycline 100mg twice daily for 14 days led to complete resolution of the endoscopic findings confirmed after 3 months of follow-up. Endoscopic findings, histology, diagnosis and treatment of this condition are discussed.
Keywords: Rectosigmoiditis; Chlamydia trachomatis; Rectitis; Sexually transmitted infections.
Abbreviations: STIs: Sexually Transmitted Infections; HIV: Human Immunodeficiency Virus; MSM: Men Who Have Sex With Men; ESR: Erythrocytes Sediment Rate; RPR: Rapid Plasma Regain; LGV: Lymphogranuloma Venereum; IBD: Inflammatory Bowel Disease;
Citation: Tsomidis I, Kouroumalis E. Chlamydia trachomatis: An unusual cause of rectosigmoiditis. J Clin Images Med Case Rep. 2024; 5(5): 3072.
Introduction
Sexually Transmitted Infections (STIs) are increasingly reported mainly those caused by Neisseria gonorrhoeae, Treponema pallidum and Chlamydia trachomatis particularly the serotypes L1, L2 and L3 that may lead to lymphogranuloma venereum [1, 2]. Risk factors are people harboring the Human Immunodeficiency Virus (HIV) or those using pre-exposure prophylaxis to prevent HIV [3,4]. Increased incidence is also observed in men who have sex with men (MSM), and people with multiple sexual partners [1,5,6]. In the bowel STIs are usually presented as Infectious Proctitis (IP), defined as inflammation of the rectum that may also be associated with inflammatory bowel disease [7,8]. Co-infection by 2 or more agents is described in 10% of MSM with IP [9-11]. Clinical, endoscopic, and histological presentation of infectious and noninfectious proctitis are similar. Inflammatory Bowel Disease (IBD) limited to the rectum and proctitis related to C. trachomatis infection may therefore be easily misdiagnosed [12-14]. The final diagnosis of these infections requires cultures, serological studies or DNA amplification tests, whereas the serological test in the case of chlamydia do not discriminate an old infection from a recent one [5] and the molecular tests are not widely available. Consequently, STI proctitis usually is managed with empirical therapy [9]. Here, we report a case of a young man with chlamydia inflammation extending beyond the rectum into the sigmoid colon who refused to have sex with another man.
Case report
A 29-year-old male patient was presented with a 30-day history of bloody diarrhea and tenesmus without other systemic symptoms. Medical, family and drug history were unremarkable. On physical examination, his abdomen was soft. The liver and spleen were not palpable and no palpable lymph nodes were found. Hemorrhoids were observed on the rectal examination. Routine laboratory studies were as follows and are summarized in Table 1 white blood cell count, 7,490/mm3 with 35% neutrophils and 53% lymphocytes; hemoglobin, 13.1 g/dL; platelets, 186.000/mm3; blood urea nitrogen, 9.8 mg/dL; creatinine, 0.9 mg/dL; C-reactive protein within normal values; ESR: 5 mm/hr. HIV testing was negative as well as testing for IgA deficiency. No Shigella or Salmonella was grown from the stool culture and Clostridium difficile toxins were not identified. Campylobacter ssp and Yersinia cultures were negative.
Table 1: The course of endoscopic treatments.
| Laboratory test | Value (Normallimits) |
|---|---|
| Leukocytes | 7.49x103/ml(4-10x103/ml)-35% neutrophils, 53% lymphocytes |
| Hemoglobin | 13.1 gr/dl(12.2-17.1 g/dl) |
| Platelets | 186x103/ml(150-400x103/ml) |
| ESR | 5 mm/h (0-15mm/h) |
| Blood ureanitrogen | 9.8 mg/dl (7-20mg/dl) |
| Creatinine | 0.9 mg/dl(0.7-1.3 mg/dl) |
| CRP | 0.8 mg/dl (0.3-1mg/dl) |
| IgA in Serum | 5.17 g/L (0.7-4g/L) |
| Stool culture | Negative forShigella, Salmonella, Yersinia, Campylobacter, Clostridium difficile toxins |
| Treponemapallidum IgM, IgG | Negative |
| RPR | Negative |
| Chlamydiatrachomatis IgA | 250 (>11titer positive) |
| Chlamydiatrachomatis IgG | 250 (>11titer positive) |
| Culture ofurogenital tract samples | Negative forCandida spp, Mycoplasma hominis, Ureoplasma urealyticum |
| HIV | negative |
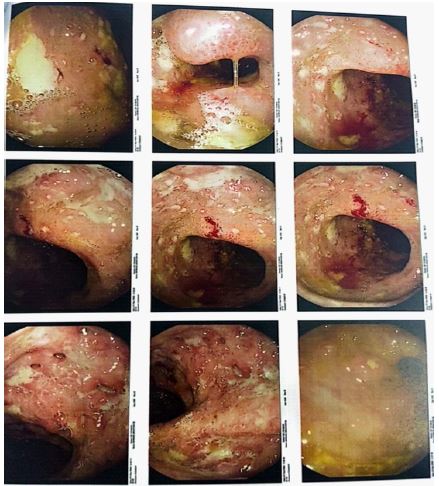
Ileocolonoscopy detected recto-sigmoidal inflammation with edema and mucosal friability accompanied by rectal and sigmoid ulcers surrounded by raised margins (Figure 1).
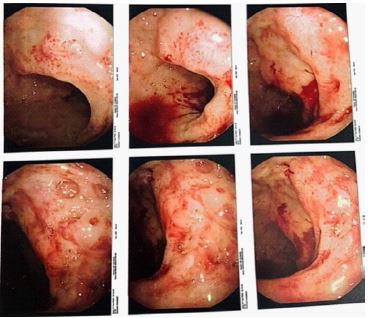
Histological examination showed minor derangement of the crypt architecture with normal mucus and edema and moderate inflammation of the submucosa. The infiltrate was patchy and consisted of lymphocytes, neutrophils, plasmacytes and eosinophils. Several crypt abscesses were found. Erosions of the epithelium were also found. The findings were considered as compatible with IBD, possibly Crohn’s disease. The patient was initially treated with ciprofloxacin 500 mg b.i.d and metronidazole 500 mg t.i.d for 2 weeks without significant improvement. Treatment with mesalazine suppositories 2 gr daily for 3 weeks was also ineffective. Sigmoidoscopy showed no signs of healing (Figure 2).
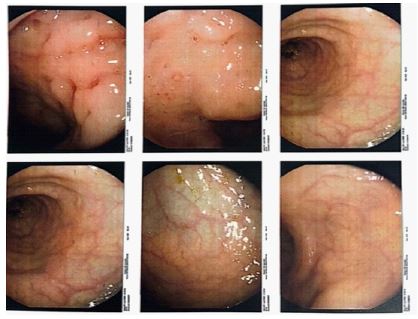
The histological examination showed colon mucosa with patchy prominent lymphoid aggregates. The lamina propria was infiltrated with mononuclear cells. At one area over a lymphoid aggregate ulceration is noted with regenerated epithelium on both sides (Aphthous ulcer). PAS Stain was negative for intranuclear inclusion. Findings were compatible with IBD. Seropositivity for T. pallidum was negative. Rectal swabs for N. Gonorrhoeae were negative and cultures for Candida spp, Mycoplasma hominis and Ureoplasma urealyticum were negative. However, seropositivity for C. trachomatis was detected, with IgA and IgG antibodies positive leading to a diagnosis of Lymphogranuloma venereum recto-sigmoiditis. No serovars were identified. The patient persistently refused having sex with other men or multiple sexual partners despite persistent interrogation. Doxycycline 100 mg b.i.d was given orally for 14 days followed by complete clinical remission. Sigmoidoscopy done two months later revealed significant improvement (Figure 3).
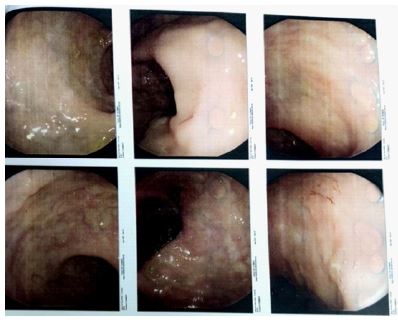
The latest sigmoidoscopy done 6 months later, showed complete remission in accordance with patient’s status, who reported formed stools without any mucus or bleeding (Figure 4).
Discussion
Infection by C. trachomatis is the commonest STI worldwide, with over 100 million people diagnosed each year [15] with an increasing incidence over the last decades [16]. The incubation period is 7-10 days usually after a receptive anal intercourse. Women with chlamydial urethritis or cervicitis may suffer from rectal infection due to direct spreading [17]. Serotypes of C. trachomatis cause several sexually transmitted diseases, such as cervicitis, endometritis, urethritis (serotypes D-K), and the commonest etiology of infectious blindness, trachoma endemicum (serotype A-C). All 15 serovars of C. trachomatis can cause proctitis. Whereas non-Lymphogranuloma Venereum (LGV) proctitis caused by serovars A-K produces mild inflammation confined to the rectal mucosa and causes few or no symptomatic infections. LGV proctitis, also called Nicolas-Favre disease, caused by serovars L1-3 produces more severe inflammation [18-20]. L1-L3 serovars are found mostly in HIV-positive patients and are often associated with other STIs [19,21]. Non-LGV serovars cause inflammation of the epithelium and are usually asymptomatic. Symptomatic patients may present with anal pain, mucopurulent or bloody discharge and tenesmus [7] as did our patient. LGV is an invasive and systemic infection. The clinical presentation of LGV may be divided into 3 stages. The first stage consists of a small painless papule, pustule, and small herpetiform ulcer usually healed within 1 week, and often not diagnosed. When proctitis is the primary manifestation of the infection, symptoms are characterized by severe anorectal pain, rectal haemopurulent discharge, and bleeding, associated with tenesmus and constipation due to mucosal and perirectal edema. Painful inguinal or femoral lymphadenopathy is typical of the second stage of infection. Mucopurulent or bloody discharge, anal pain, malaise, myalgia, and fever are symptoms of this stage. If left untreated, the third stage is associated with the appearance of rectal abscesses, granulomas, fistulae, and strictures [7]. During this stage, LGV proctitis may mimic rectal Crohn’s disease. Our patient consistently denied any sexual contact with other men and was negative for HIV infection and tests for gonorrhea and syphilis. This is uncommon today, but transmission may happen through any unprotected intercourse. The initial papules are non-tender and usually undetected making the transmission easy at this stage. Moreover, females may be asymptomatic carriers [22]. Endoscopic findings of chlamydial proctitis range from mild erythematous and friable mucosa to ulcers or granulomas with mucopurulent exudates [23]. These endoscopic findings may be difficult to differentiate from IBD [7,24,25]. This was the case in the first endoscopic examin tion of our patient. Multiple discontinuous ulcers in the rectum, similar to our patients are frequently reported in chlamydia related proctitis [23,26,27]. Another unusual endoscopic finding is a pseudo-tumor lesion. This is more frequently related to LGV and is described as a friable ulcerated multilobular mass that may occupy the entire rectal circumference [28-31]. The histological examination shows a lymphoplasmacytic infiltrate with gland architectural distortion and decreasing of mucus secretion findings consistent with IBD [25,31]. However, neutrophil infiltration can be found in all patients including the presence of cryptitis and microabscess in some of them. The presence of neutrophils and/or cryptitis should lead to a possible diagnosis of chlamydial infection [32-34]. Macrophage infiltration forming incomplete granulomas is also a prominent finding [31,33,35]. Exclusion of Crohn’s disease and tuberculosis should be ruled out in these cases. However, even if granulomas often differ between CD and LGV [36] it should be kept in mind that pathognomonic features of LGV do not exist. The pathological findings of LGV proctitis are easily misinterpreted even by experienced pathologists [7,37,38] and clinical suspicion is important for patients at risk for STI. This was indeed the case with our patient. The first biopsy was misinterpreted as IBD and only when the initial treatment failed, the findings were reconsidered as suggested for clinical diagnosis of LGV [12]. The other diagnostic hints that should lead to the clinical diagnosis of LGV colitis over IBD are a history of MSM or travel and resolution of symptoms with antibiotics. Complete resolution of endoscopic findings by the proper antibiotics confirmed the diagnosis in our case [12, 39]. However, nucleic acid amplification tests are the gold standard for the diagnosis of Chlamydia and the identification of the specific chlamydia serovars L1, L2 and L3. The L2 serovar is the most prevalent serovar identified in recent epidemic outbreaks [40]. Immunohistochemistry may be useful in diagnosis demonstrating staining for Chlamydia trachomatis in the cytoplasm of macrophages [41] but is not so sensitive as the amplification tests [31,34]. It is suggested that all patients with IBD in the colorectal tract confirmed by endoscopy and histopathology, should be tested for STIs using sensitive methodologies [42]. Amplification tests were not available in our case, so that the identification of the particular serovar was not possible. Serological tests, the response to treatment and a long over six months follow-up, were robust criteria for diagnosis in our case. Doxycycline 100 mg twice daily for 7 days is recommended as the first line of treatment with azithromycin 1 gr once orally as an alternative treatment Azithromycin 1 gr once, orally is the recommended treatment in pregnancy. An extended course of doxycycline for 21 days is recommended if there is clinical suspicion of LGV [5,10,43]. Levofloxacin 500 mg daily for 7 days is also recommended as alternative [44]. Empirical treatment of genital herpes should also be considered in cases of painful ulcers and among patients with HIV [5,10]. Doxycycline is the preferred treatment over azithromycin as a result of a systematic review and meta-analysis that demonstrated significantly less failures with doxycycline particularly among men with rectal chlamydia [45,46]. It is advisable therefore, that single-dose azithromycin should be preferred only when doxycycline cannot be used.
References
- Tuddenham S, Hamill MM, Ghanem KG. Diagnosis and Treatment of Sexually Transmitted Infections: A Review. JAMA. 2022; 327: 161-172.
- Lamb CA, Lamb EI, Mansfield JC, Sankar KN. Sexually transmitted infections manifesting as proctitis. Frontline Gastroenterol. 2013; 4: 32-40.
- Nguyen VK, Greenwald ZR, Trottier H, Cadieux M, Goyette A, Beauchemin M, et al. Incidence of sexually transmitted infections before and after preexposure prophylaxis for HIV. AIDS. 2018; 32: 523-530.
- Traeger MW, Cornelisse VJ, Asselin J, Price B, Roth NJ, Willcox J, et al. Association of HIV Preexposure Prophylaxis With Incidence of Sexually Transmitted Infections Among Individuals at High Risk of HIV Infection. JAMA. 2019; 321: 1380-1390.
- Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021; 70: 1-187.
- Newman L, Rowley J, Vander Hoorn S, Wijesooriya NS, Unemo M, Low N, et al. Global Estimates of the Prevalence and Incidence of Four Curable Sexually Transmitted Infections in 2012 Based on Systematic Review and Global Reporting. PLoS One. 2015; 10: e0143304.
- Hoentjen F, Rubin DT. Infectious proctitis: when to suspect it is not inflammatory bowel disease. Dig Dis Sci. 2012; 57: 269-273.
- Rizza S, Mistrangelo M, Ribaldone DG, Morino M, Astegiano M, Saracco GM, et al. Proctitis: a glance beyond inflammatory bowel diseases. Minerva Gastroenterol Dietol. 2020; 66: 252-266.
- Klausner JD, Kohn R, Kent C. Etiology of clinical proctitis among men who have sex with men. Clin Infect Dis. 2004; 38: 300-302.
- de Vries HJC, Nori AV, Kiellberg Larsen H, Kreuter A, Padovese V, Pallawela S, et al. 2021 European Guideline on the management of proctitis, proctocolitis and enteritis caused by sexually transmissible pathogens. J Eur Acad Dermatol Venereol. 2021; 35: 1434-1443.
- Kumar N, Bahadur T, Agrawal SK. Concurrent syphilis and Chlamydia trachomatis infection in bisexual male: A rare case of proctitis. J Family Med Prim Care. 2019; 8: 1495-1496.
- Gallegos M, Bradly D, Jakate S, Keshavarzian A. Lymphogranuloma venereum proctosigmoiditis is a mimicker of inflammatory bowel disease. World J Gastroenterol. 2012; 18: 3317-3321.
- Lee KJ, Kim J, Shin DH, Jung JO, Koh S, Kim KY, et al. Chlamydial Proctitis in a Young Man Who Has Sex with Men: Misdiagnosed as Inflammatory Bowel Disease. Chonnam Med J. 2015; 51: 139-141.
- Neri B, Stingone C, Romeo S, Sena G, Gesuale C, Compagno M, et al. Inflammatory bowel disease versus Chlamydia trachomatis infection: a case report and revision of the literature. Eur J Gastroenterol Hepatol. 2020; 32: 454-457.
- Lanjouw E, Ouburg S, de Vries HJ, Stary A, Radcliffe K, Unemo M. 2015 European guideline on the management of Chlamydia trachomatis infections. Int J STD AIDS. 2016; 27: 333-348.
- 16. Somayaji R, Naugler C, Guo M, Church D. Examining Chlamydia trachomatis and Neisseria gonorrhoeae rates between 2010 and 2015: a population-based observational study. Int J STD AIDS. 2017; 28: 822-828.
- Cone MM, Whitlow CB. Sexually transmitted and anorectal infectious diseases. Gastroenterol Clin North Am. 2013; 42: 877-892.
- Quinn TC, Goodell SE, Mkrtichian E, Schuffler MD, Wang SP, Stamm WE, et al. Chlamydia trachomatis proctitis. N Engl J Med. 1981; 305: 195-200.
- Martin-Iguacel R, Llibre JM, Nielsen H, Heras E, Matas L, Lugo R, et al. Lymphogranuloma venereum proctocolitis: a silent endemic disease in men who have sex with
- de Vries HJ, Smelov V, Middelburg JG, Pleijster J, Speksnijder AG, Morré SA. Delayed microbial cure of lymphogranuloma venereum proctitis with doxycycline treatment. Clin Infect Dis. 2009; 48: e53-56.
- White JA. Manifestations and management of lymphogranuloma venereum. Curr Opin Infect Dis. 2009; 22: 57-66.
- O’Byrne P, MacPherson P, DeLaplante S, Metz G, Bourgault A. Approach to lymphogranuloma venereum. Can Fam Physician. 2016; 62: 554-558.
- López-Vicente J, Rodríguez-Alcalde D, Hernández-Villalba L, Moreno-Sánchez D, Lumbreras-Cabrera M, Barros-Aguado C, et al. Proctitis as the clinical presentation of lymphogranuloma venereum, a re-emerging disease in developed countries. Rev Esp Enferm Dig. 2014; 106: 59-62.
- Sigle GW, Kim R. Sexually transmitted proctitis. Clin Colon Rectal Surg. 2015; 28: 70-78.
- Santos AL, Coelho R, Silva M, Rios E, Macedo G. Infectious proctitis: a necessary differential diagnosis in ulcerative colitis. Int J Colorectal Dis. 2019; 34: 359-362.
- Gopal P, Shah RB. Primary Anal Canal Syphilis in Men: The Clinicopathologic Spectrum of an Easily Overlooked Diagnosis. Arch Pathol Lab Med. 2015; 139: 1156-1160.
- Garg I, Thoendel MJ, Goenka AH. Lymphogranuloma Venereum Proctitis. Clin Gastroenterol Hepatol. 2017; 15: A29-A30.
- Dhawan B, Makharia GK, Juyal D, Sebastian S, Bhatia R, Khanna N. Chlamydia trachomatis proctitis masquerading as carcinoma rectum: First case report from India. Indian J Pathol Microbiol. 2017; 60: 259-261.
- Taylor G, Dasari BV, McKie L, Harvey C, Emerson C. Lymphogranuloma venerum (LGV) proctitis mimicking rectal cancer. Colorectal Dis. 2011; 13: e63-64.
- García-Mayor Fernández RL, Fernández González M, Martínez-Almeida Fernández R. Atypical lymphogranuloma venereum mimicking an anorectal neoplasm. Rev Esp Enferm Dig. 2018; 110: 676-677.
- Arévalo F, Rayme S, Zurita F, Ramírez R, Franco D, Montes P, et al. Immunohistochemical detection of chlamydia trachomatis in sexually transmitted infectious proctitis. BMC Gastroenterol. 2022; 22: 171.
- Arnold CA, Limketkai BN, Illei PB, Montgomery E, Voltaggio L. Syphilitic and lymphogranuloma venereum (LGV) proctocolitis: clues to a frequently missed diagnosis. Am J Surg Pathol. 2013; 37: 38-46.
- Soni S, Srirajaskanthan R, Lucas SB, Alexander S, Wong T, White JA. Lymphogranuloma venereum proctitis masquerading as inflammatory bowel disease in 12 homosexual men. Aliment Pharmacol Ther. 2010; 32: 59-65.
- Levy I, Gefen-Halevi S, Nissan I, Keller N, Pilo S, Wieder-Finesod A, et al. Delayed diagnosis of colorectal sexually transmitted diseases due to their resemblance to inflammatory bowel diseases. Int J Infect Dis. 2018; 75: 34-38.
- Van Kruiningen HJ, Hayes AW, Garmendia A, Cui J, de Abreu FB, Tsongalis GJ, et al. Evidence for Chlamydia in Crohn’s disease. Int J Dig Dis. 2016; 2: 1.
- Gomollón F, Dignass A, Annese V, Tilg H, Van Assche G, Lindsay JO, et al. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical Management. J Crohns Colitis. 2017; 11: 3-25.
- Høie S, Knudsen LS, Gerstoft J. Lymphogranuloma venereum proctitis: a differential diagnose to inflammatory bowel disease. Scand J Gastroenterol. 2011; 46: 503-510.
- Di Altobrando A, Tartari F, Filippini A, D’Antuono A, Patrizi A, Filippi F, et al. Lymphogranuloma venereum proctitis mimicking infammatory bowel diseases in 11 patients:
- Arnold CA, Roth R, Arsenescu R, Harzman A, Lam-Himlin DM, Limketkai BN, et al. Sexually transmitted infectious colitis vs inflammatory bowel disease: distinguishing features from a case-controlled study. Am J Clin Pathol. 2015; 144: 771-781.
- Hamlyn E, Taylor C. Sexually transmitted proctitis. Postgrad Med J. 2006; 82: 733-736.
- Borel N, Marti H, Pospischil A, Pesch T, Prähauser B, Wunderlin S, et al. Chlamydiae in human intestinal biopsy samples. Pathog Dis. 2018; 76: fty081.
- Siwak E, Suchacz MM, Cielniak I, Kubicka J, Firląg-Burkacka E, Wiercińska-Drapało A. Inflammatory Bowel Disease in Adult HIV-Infected Patients-Is Sexually Transmitted Infections Misdiagnosis Possible? J Clin Med. 2022; 11: 5324.
- Coelho R, Ribeiro T, Abreu N, Gonçalves R, Macedo G. Infectious proctitis: what every gastroenterologist needs to know. Ann Gastroenterol. 2023; 36: 275-286.
- Van Ommen CE, Malleson S, Grennan T. A practical approach to the diagnosis and management of chlamydia and gonorrhea. CMAJ. 2023; 195: E844-E849.
- Kong FY, Tabrizi SN, Law M, Vodstrcil LA, Chen M, Fairley CK, et al. Azithromycin versus doxycycline for the treatment of genital chlamydia infection: a meta-analysis of randomized controlled trials. Clin Infect Dis. 2014; 59: 193-205.
- Páez-Canro C, Alzate JP, González LM, Rubio-Romero JA, Lethaby A, Gaitán HG. Antibiotics for treating urogenital Chlamydia trachomatis infection in men and non-pregnant women. Cochrane Database Syst Rev. 2019; 1: CD010871.