Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Acute promyelocytic leukemia advances under cover during immunophenotyping
Clément Burgy1; François Vergez1,2,3*; Alban Canali1,2,3
1Hematology Laboratory, Toulouse University Hospital Center, University Cancer Institute of Toulouse Oncopole, Toulouse, France.
2Toulouse III Paul Sabatier University, Toulouse, France.
3Cancer Research Center of Toulouse, UMR1037 INSERM, ERL5294 CNRS, Toulouse, France.
*Corresponding Author : François Vergez
Hematology Laboratory, Toulouse University Hospital Center, University Cancer Institute of Toulouse Oncopole, Toulouse, France.
Email: Vergez.Francois@iuct-oncopole.fr
Received : Apr 28, 2024
Accepted : May 17, 2024
Published : May 24, 2024
Archived : www.jcimcr.org
Copyright : © Vergez F (2024).
Citation: Burgy C, Vergez F, Canali A. Acute promyelocytic leukemia advances under cover during immunophenotyping. J Clin Images Med Case Rep. 2024; 5(5): 3073.
Description
A 53-year-old woman, with no notable medical history, presented with intraoral hemorrhagic bubbles. Her full blood count showed severe thrombocytopenia (platelets 75×109/L) and leukocytosis (WBC 59,5×109/L), but no anemia (hemoglobin concentration 121g/L).
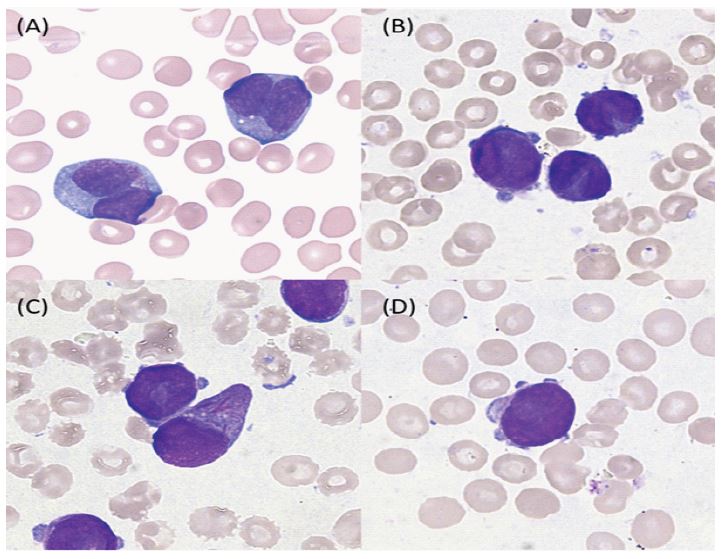
Microscopic examination of the blood film revealed 96% big size blasts (Figure 1A) with intermediate nuclear-cytoplasmic ratio, irregular nucleus majoritary binucleate, intermediate chromatin and basophilic agranular cytoplasm. Thus, hydroxyurea was initially administrated to reduce white blood cells. A bone marrow aspirate showed 93% leukemic cells composed of abnormal promyelocytes with butterfly-shaped nucleus (Figure 1B and 1C, left), abnormal hypergranular promyelocytes with single Auer rods or very rarely in bundles (Figure 1C, right) and myeloblasts with cytoplasmic expansions (Figure 1D). These observations suggest Acute Promyelocytic Leukaemia (APL), microganular form.
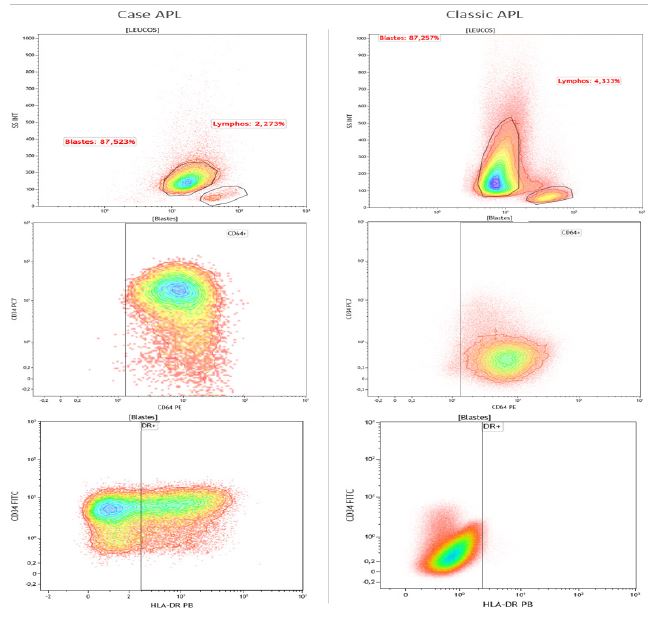
However, immunophenotyping by flow cytometry of bone marrow (Figure 2) has cast doubt on the diagnosis, showing 87,5% blasts with decreased expression of CD45 and low Side Scatter (SS). Surprisingly, immature marker CD34 was positive and 61% blasts expressed HLA-DR, which goes against the cytological hypothesis, APL are known to be at an advanced stage of maturation with loss of these immaturity markers and strong SS. The only typical expression is that of CD64.
Cytogenetic analysis revealed karyotype with translocation t(15;17) associated to unbalanced translocation t(2;8) resulting in trisomy 8q. Molecular analysis detected a short (S-,bcr3) PML::RARA transcript form with two FLT3 internal duplications including one subclonal. Following these results, the diagnosis of acute promyelocytic leukemia with t(15;17)/PML::RARA fusion was formally established.
Double induction therapy with retinoic acid Idarubicin was immediately administrated following blood film examination. Arsenous acid was administrated on the 9th day. A progressive decrease in leukocytosis and blasts was observed, leading to leukopenia (WBC 1,4 G/L) on the 4th day.
Although the immunophenotyping of APL is now well known, this case shows that in very rare cases it may correspond to a phenotype of immature myeloblasts rather than promyelocytes, and should not derail the diagnosis, particularly in this life-threatening hemopathy.