
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Gram negative osteoarticular infections: An observational study over one year
Aashna Gandhi1*; Geethu Joe2; Rajeev Soman1
1Department of Infectious Diseases, Jupiter Hospital, Pune, India.
2Department of Microbiology, Jupiter Hospital, Pune, India.
*Corresponding Author : Aashna Gandhi
Department of Infectious Diseases, Jupiter Hospital, Pune, India.
Tel: +919870018310;
Email: aashnagandhi2206@gmail.com
Received : May 01, 2024
Accepted : May 17, 2024
Published : May 24, 2024
Archived : www.jcimcr.org
Copyright : © Gandhi A (2024).
Citation: Gandhi A, Joe G, Soman R. Gram negative osteoarticular infections: An observational study over one year. J Clin Images Med Case Rep. 2024; 5(5): 3074.
Background
Osteoarticular infections form an important part of orthopedic & infectious disease practice. Currently, gram negative infections have become increasingly important. Therefore we analyzed the gram negative osteoarticular infections at our institute with respect to the causative organisms, antibiotic susceptibility, treatment used and outcome.
Methodology
This is an observational study at a tertiary care center in Pune, India. 37 consecutive patients of bone and joint infections (which included native joint septic arthritis, periprosthetic joint infections, spine infections and osteomyelitis) from 1st January 2022 to 31st December 2022 were included. There were total 19 gram negative infections, 17 of which were identified by culture and 2 patients where cultures were repeatedly negative and the organism was identified only via 16S RNA sequencing or Multiplex PCR. Antibiotic susceptibility, treatment used and outcome was studied for all patients.
Results
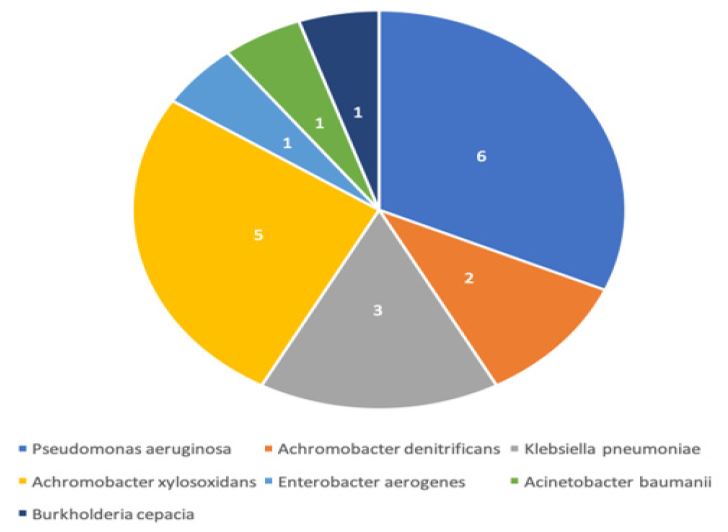
19 samples (16 Gram negative monomicrobial and 3 polymicrobial which also had gram negative organisms) were derived from 9 patients who were male and 10 were female. 10 patients were above the age of 65. There were 8 knee prosthetic joint infections, 5 infective spondylodiscitis, 2 septic arthritis, 2 fracture related implant infections, 1 hip prosthetic joint infection and 1 chronic osteomyelitis. The types of organisms found are shown in Figure 1.
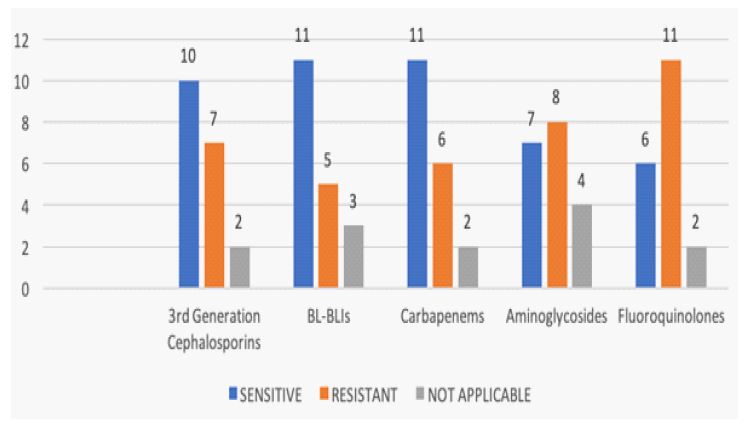
The novel modality of Joint infection Multiplex PCR panel was employed for 1 sample - which detected Pseudomonas aeruginosa, while for 2 samples, identification was carried out by 16S RNA sequencing - which detected Acinetobacter baumanii in 1 sample and Achromobacter xylosoxidans in the other. 7 of the 19 organisms were resistant to 3rd generation cephalosporins, 5 were resistant to Beta-lactam/Beta-lactamase inhibitor (BL-BLIs), 6 were resistant to carbapenems, 8 were resistant to aminoglycosides and 11 were resistant to fluoroquinolones. A detailed susceptibility pattern of all the organisms is shown in Figure 2.
Table 1: The course of endoscopic treatments.
| SR NO | DIAGNOSIS | ORGANISM | ANTIBIOTICS | SURGICAL INTERVENTION | OUTCOME |
|---|---|---|---|---|---|
| 1 | L5-S1 disc prolapse withlarge epidural abscess with spondylodiscitis (post injection) | Pseudomonas aeruginosa | Inj Ceftazidime 2 g IVtid + Inj Amikacin 1 g IV od for 6 weeks | L5-S1 lumbar decompression + discectomy +fusion | Good |
| 2 | Lumbar canal stenosisL3-S1 with grade 1 degenerative spondylolisthesis L4-5 (post op infection) | Achromobacter denitrificans | Tab levofloxacin 500 mgod + Tab minocycline 100 mg bid; did not tolerate minocycline so changed totab co-trimoxazole (800/160) tid and Inj meropenem 1 g iv tid was also givenfor 15 days | None, implant retained | Good |
| 3 | Right knee septicarthritis (post liver transplant, biliary stricture + bacteremia) | Klebsiella pneumoniae | Inj ceftazidime-avibactam2.5 g tid + Inj aztreonam 2 g tid x 6 weeks; multiple courses | Multiple aspirations + joint lavage | Failed |
| 4 | Bilateral knee - totalknee replacement – periprosthetic joint infection | Achromobacter denitrificans | Tab levofloxacin 500 mgod + Tab minocycline 100 mg bid for a long time, still under treatment | None, implants retained | Good |
| 5 | Left knee septicarthritis | Pseudomonas aeruginosa | Tab ciprofloxacin 500 mgbid for a long time, still under treatment | Joint lavage | Good |
| 6 | Left knee - total kneereplacement – periprosthetic joint infection | Achromobacter xylosoxidans | Tab minocycline 100 mgbid for a long time, still under treatment | None, implant retained | Good |
| 7 | Left hip - total hipreplacement – periprosthetic joint infection | Enterobacter aerogenes, Kocuria kristinae | Tab ciprofloxacin 500 mgbid for a long time, still under treatment | None, implant retained | Good |
| 8 | Right knee total kneereplacement – periprosthetic joint infection | MRSA, Klebsiella pneumoniae | Inj Ceftazidime-avibactam2.5 g tid + aztreonam 2 g tid + Inj Teicoplanin 400 mg iv od for 3 months | None, implant retained | Lost to follow up |
| 9 | TI1 fracture withimplants insitu with non healing wound | Acinetobacter baumanii | Tab minocycline 100 mgbid x 6 weeks | Implants removed | Good |
| 10 | Grade 3 compound fractureof the tibia | Enterococcus faecalis, Pseudomonas aeruginosa | Inj ceftazidime +avibactam 2.5 g tid + aztreonam 2 g tid + Inj ampicillin 2 g IV qid for 6weeks | Implants removed | Good |
| 11 | Chronic osteomyelitis ofleft tibia | Pseudomonas aerugonisa | Tab ciprofloxacin 750 mgbid for 6 weeks | None | Good |
| 12 | Left knee - total kneereplacement – periprosthetic joint infection | Burkholderia cepacia | Inj ceftazidime 2 g ivtid + tab minocycline 100 mg bid for a long time | None, implant retained | Lost to follow up |
| 13 | Right knee - total kneereplacement – periprosthetic joint infection | Achromobacter xylosoxidans | Tab minocycline 100 mgbid for a long time | None, implant retained | Lost to follow up |
| 14 | Infectivespondylodiscitis | Pseudomonas aeruginosa | Tab ciprofloxacin 500 mgbid for 8 weeks | Lost to follow up | Lost to follow up |
| 15 | L5-S1 discectomy /laminectomy - stabilization (post op infection) | Pseudomonas aeruginosa | Tab ciprofloxacin 750 mgbid for a long time | Lost to follow up | Lost to follow up |
| 16 | Left knee - total kneereplacement – periprosthetic joint infection | Achromobacter xylosoxidans | Tab co-trimoxazole(800/160) tid | None, implant retained | Good |
| 17 | Spinal fixation (post opinfection) | Klebsiella pneumoniae | Inj cefazidime-avibactam2.5 g IV tid + Inj aztreonam 2 g IV tid for 8 weeks | Lost to follow up | Lost to follow up |
| 18 | Right knee - total kneereplacement – periprosthetic joint infection | Achromobacter xylosoxidans | Inj ceftazidime 2 g IVtid for 6 weeks + Tab minocycline 100 mg bid | None, implant retained | Failed |
| 19 | Left knee - total kneereplacement – periprosthetic joint infection | Achromobacter xylosoxidans | Lost to follow up | Lost to follow up | Lost to follow up |
OD: Once a day; Bid: Twice a day; Tid: Thrice a day; Qid: Four times a day.
Of the 6 carbapenem resistant organisms, 3 were Klebsiella pneumoniae, 2 were Achromobacter xylosoxidans, and 1 was Pseudomonas aeruginosa. Xpert CARBA-R test was performed on 2 of the Klebsiella pneumoniae isolates, which revealed presence of NDM+OXA-48 like carbapenemases. Ceftazidime-avibactam + Aztreonam synergy test was performed for 3 of the organisms and it showed positive synergy. The detailed information of the diagnosis, organism, treatment given and outcome is shown in Table 1. 10 of the patients in our study had a good outcome, 2 failed and required re-treatment. 8 patients are still under treatment and 7 were lost to follow up.
Discussion
Osteoarticular infections including septic arthritis, periprosthetic joint infections, osteomyelitis and spinal infections cause significant morbidity and mortality, as well as a burden on healthcare. Often, these infections are nosocomial and caused by Multi-Drug Resistant (MDR) organisms. The presence of foreign bodies like implants and prosthesis add to the challenges due to biofilm formation and the need for removal of the same. Data from the Western World suggests that gram positive organisms like Staphylococcus aureus and coagulase negative Staphylococci [1,2] are important causes, but as our study reveals, gram negative organisms are equally important causes of osteoarticular infections in India. This poses a significant challenge due to the antimicrobial resistance of these organisms. In our study, the most common causative organism was Pseudomonas aeruginosa. 11 organisms in our study were MDR; 6 were carbapenem resistant. Similar results are seen in other studies from India [3]. 3 of the carbapenem resistant organisms were Klebsiella pneumoniae, out of which the Xpert CARBA-R test was performed on 2 isolates, where both NDM+OXA-48 like carbapenemases were found. Synergy testing with ceftazidime-avibactam + aztreonam was positive for all the Klebsiella isolates. However, this test was not performed for the other carbapenem resistant isolates. The limitations of this study include a small sample size, unavailability of susceptibility data for some isolates and lack of information about the outcome of some of the patients.
It is important to know local epidemiology of antimicrobial resistance, as it helps guide the clinicians in deciding empiric antibiotics while waiting for culture results. In cases where cultures do not grow an organism, multiplex PCRs and 16S RNA sequencing may be used to reveal the causative organisms, but the susceptibility of the same remains unknown. Besides, the true significance of sequencing results is somewhat difficult to ascertain at present. Our study had 2 patients where cultures were repeatedly negative, the organism was discovered via 16S RNA sequencing and antibiotics were chosen based on local epidemiological data.
Conclusion
Contrary to the Western data, Indian data shows a significant proportion of Gram negative organisms in osteoarticular infections. MDR gram negative organisms, especially carbapenem resistant pose an immense challenge in diagnosis and management. This study highlights the need for large scale as well as repeated studies to provide clinicians the guidance that they need.
References
- Berendt T, Byren I. Bone and joint infection. Clinical medicine. 2004; 4(6): 510.
- Benito N, Franco M, Ribera A, Soriano A, Rodriguez-Pardo D, et al. Time trends in the aetiology of prosthetic joint infections: A multicentre cohort study. Clinical Microbiology and Infection. 2016; 22(8): 732-e1.
- Menon A, Bhadiyadra R, Kuntwad V, Soman R, Rodrigues C, et al. Infection after osteosynthesis: Good results in bad bugs. InOrthopaedic Proceedings. The British Editorial Society of Bone & Joint Surgery. 2019; 101(14): 44.