
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Transoral resection and reconstruction of hypopharyngeal liposarcoma
Meltem Bozaci Kiliçoğlu1*; Günter Hafiz2
1Otorhinolaryngology-Head and Neck Surgery, Yeditepe University Koşuyolu Hospital, Istanbul, Turkey.
2Otorhinolaryngology-Head and Neck Surgery, Private Practice, Istanbul, Turkey.
*Corresponding Author : Meltem B Kiliçoğlu
Otorhinolaryngology-Head and Neck Surgery, Yeditepe University Koşuyolu Hospital, Istanbul, Turkey.
Tel: +90-554-510-38-09;
Email: meltembozaci@gmail.com
Received : May 01, 2024
Accepted : May 21, 2024
Published : May 28, 2024
Archived : www.jcimcr.org
Copyright : © Kiliçoğlu MB (2024).
Abstract
Hypopharyngeal and esophageal liposarcoma are rare malignant tumors. Low grade liposarcoma have similarities to lipoma. Surgical resection with endoscopic or cervical approach is treatment option. We present hypopharyngeal liposarcoma that was treated with endoscopic resection and reconstruction.
Keywords: Hypopharynx; Liposarcoma; Endoscopic; Free flap; Low grade.
Citation: Kiliçoğlu MB, Hafiz G. Transoral resection and reconstruction of hypopharyngeal liposarcoma. J Clin Images Med Case Rep. 2024; 5(5): 3078.
Introduction
Liposarcomas are rare malignant tumors. Head and neck sarcomas constitute 5-10% of all sarcomas in adults and 35% of all sarcomas in pediatric population. It involves frequently retroperitoneum, trunk, and extremites [1]. Hypopharyngeal and esophageal liposarcoma were seen as extremely rare and Mansour et al. described the first case in the literature as pedunculated esophageal liposarcoma [2]. Less than forty cases of liposarcoma developed in the hypopharynx [3]. They look like lipomas microscopically. Four subtypes were described. Low-grade liposarcomas have the most similarities to lipoma [4]. We present this patient who is treated as transoral resection and reconstruction with a radial free flap.
Case presentation
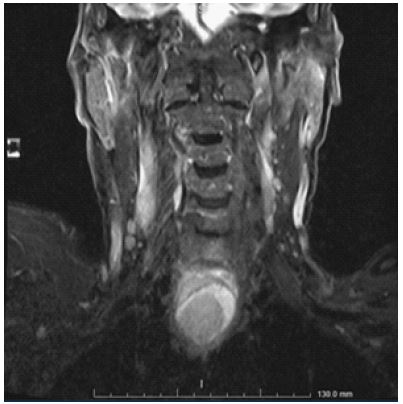
A 72-year-old man applied to another center with disphagia for 2 months and 10 kg weight loss in a month. The patient has no chronic disease. In his endoscopic examination a smooth-surfaced lesion was observed extending from the lateral wall of left pyriform sinus to the post-cricoid region. No cervical lymphadenopathy was palpable. A Computed Tomography (CT) scan and a Magnetic Resonance İmaging (MRI) was made to search this mass. In CT examination there was obliteration of the pyriform sinuses on both sides at the level of hypopharynx and an asymmetrical stenosis in the hypopharyngeal air column and soft tissue thickening extending to the prevertebral area in the posterior. A mass was observed 3,7 x 3,6 cm heterogeneous density extending to the proximal esophagus. In MRI examination the mass that started from posterior part of the supraglottic larynx level, hyperintense in T1A, heterogeneous lesion in T2A (Figure 1) with heterogeneous contrast enhancement, partially obliterated the left aryepiglottic fold and left pyriform sinus, narrowed the air column posteriorly and continued with esophagus was seen. Nodal or distant metastasis was seen in Positron Emission Tomography (PET). A biopsy was done under general anesthesia. After his pathology report was compatible with low-grade liposarcoma, he was sent to us to plan the surgery. The mass was excised with transoral diot laser endoscopically with intact margins. It was decided to perform a radial free flap for reconstruction in order to prevent postoperative mediastinitis complication. The flap was sutured endoscopically to protect the sensory nerves. Nasogastric tube was inserted to esophagus and trachetomy was done to protect the airway. After staying for one night in the intensive care unit, the patient stayed in the ward for a week. Two months later, the patient began to feed orally and was decannulated. Immunohistological reports were compatible with low-grade liposarcoma. The patient was followed up by ENT and Oncology in the next periods. Voluntary informed consent was acquired from the patient.


Discussion & conclusion
Hypopharynx is a rare site of liposarcoma. Typical symptoms of liposarcoma are dysphagia, weight loss, and foreign body sensation. Hoarseness and airway obstruction are rare symptoms. Physicians may observe nausea, vomiting, and regurgitation of food debris [5]. Flexible fiberoptic laryngoscopy make out a mass arising from piriform sinus, posterior wall of the hypopharynx or post cricoid area. Radiological investigations are necessary to determine size, location, extension of the tumor and relations with neurovascular structures. In our case, we saw dysphagia and weight loss. CT, MRI and PET were applied to guide the treatment.
Enzinger and Weis divide sarcomas into five subtypes as well differentiated, myxoid, pleomorphic, round cell and dedifferantiated [6]. Well differentiated liposarcoma accounts for about 30-40% of all liposarcomas [7]. These tumors come about aged 60 to 80 and they are seen more commonly in men. Histologic examination is important for diagnosis. Well differentiated liposarcoma resembles lipoma. Atypical cells, lipoblast, and irregular adipocyte size are important in distinguishing well-differentiated liposarcoma from benign lipomas. Most authors suggest MDM2 as it is a high specific marker for well-differentiated liposarcoma [8]. Our case was also MDM2 positive.
The tumor always was seen fixed to adjacent tissues, encapsulated and slow growing. Regional lymph node and distant metastasis are not usually presented [9]. Surgical excision was main treatment. A cervical (lateral pharyngotomy) approach and endoscopic surgery could be performed for hypopharyngeal liposarcoma. Incomplete excision is related with recurrens. Neck dissection for the treatment of lymph nodes is not necessary for the low rate of nodal metastasis. Complete surgical resection and no adjuvant treatment is recommended in well differantiated liposarcoma [10]. In our case ın PET CT distant or nodal metastasis was not observed. After the surgical treatment, there is no need for adjuvant therapy.
If the surgeon has enough experience for laser resection, this method will be successful. Laser resection suppiled fewer postoperative complications due to tracheotomy, percutaneous incisions and drains. On the other hand evaluating of margins were required experinces. As it was a large mucosal defect after the excision with laser in our case, we decided to make reconstruction with free flap.
If the margin of the tumor is seen completely, the tumor is located in hypopharynx and it is not aggressive, endoscopic resection is recommended firstly. After the excision of the tumor the mucosal defect is not large, it can be repaired with primary suturing. Thus, the patient’s hospital stay and returning to normal activities will be faster.
In conclusion, liposarcoma rarely develops in the head and neck. Surgical resection is the first treatment option. Surgical resection is usually adequate for low-grade liposarcoma. According to our experience on this case, we made endoscopic surgery to reduce the morbidities. The patient started oral feeding within 2 months. We didn’t understand why this period was longer. Our case shows that endoscopic resection may be preferred in low-grade liposarcoma and the recovery period of the patient may be prolonged in endoscopic procedures.
Declarations
Conflict of interest: There is no conflict of interest.
Funding: The authors declared that this study has received no financial support.
Author contributions: Supervision-GH; Writing Manuscript- MBK, GH; Literature Review- MBK, GH; Data Collection-MBK.
References
- Srivastava A, Ghosh A, Saha S, Saha VP, Chakraborty D. Sarcomas of head and neck. A 10 years experience. Indian J Otolaryngol Head Neck Surg. 2007; 59: 322-6.
- Mansour KA, Fritz RC, Jacobs DM, Vellios F. Pedunculated liposarcoma of the esophagus: A first case report. J Thorac Cardiovasc Surg. 1983; 86: 447-50.
- Zhu H, Sun J, Wei S, Wang D, Brandwein M. Well-differentiated laryngeal/ hypopharyngeal liposarcoma in the MDM2 era report of three cases and literature review. Head Neck Pathol. 2016; 11: 146-151.
- Luna-Ortiz K, Rodriguez-Garcia R, Lopez Basave H. Recurrent larynx and hypopharyngeal liposarcoma with systemic progression. J Clin Case Rep. 2017; 7: 12.
- Smith MA, Kluck E, Jagannath S, Yang SC. Giant multi-polypoid liposarcoma of the esophagus: An atypical presentation. Ann Thorac Surg. 2010; 89(2): 610-2.
- Enzinger FM, Weis SW. Soft tissue tumors. St Louis: Mosby. 1995; 431-66.
- Fletcher CDM, Sundaram M, Rydholm A, Coindre JM, Singer S. Soft tissue tumours: Epidemiology, clinical features, histopathological typing and grading. In: Fletcher CDM, Krishnan Unni K, Mertens F, editors. World Health Organization classification of tumours. Pathology and genetics of tumours of soft tissue and bone. Lyon: IARC Press. 2002; 12-8.
- Takano K, Kondoh A, Matsumiya H, Himi T. A well-differentiated liposarcoma of the hypopharynx. Otolaryngol Head Neck Surg. 2011; 144(3): 479-80.
- Gritli S, Khamassi K, Lachkhem A, Touati S, Chorfa A, et al. Head and neck liposarcomas: A 32 years experience. Auris Nasus Larynx. 2010; 37(3): 347-51.
- Nouri H, Hassani R, Aderdour L, Raji A. The well-differentiated liposarcoma of the hypopharynx. Eur Ann Otorhinolaryngol Head Neck Dis. 2011; 128(3): 143-5.