
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
CT guided percutaneous NBCA glue injection of rectal varices for refractory rectal variceal bleed as a bailout
Devara Anil Kashi Vishnuvardhan1*; Lavanya P2; Sandeep Botcha2; Biswa Basu Das3; Sandeep Sahu4
1Lead Consultant, Radiology and Interventional Radiology, Medicover Hospitals, MVP, Visakhapatnam, Andhra Pradesh, India.
2Consultant Interventional Radiologist, MVP Medicover Hospitals, Visakhapatnam, Andhra Pradesh, India.
3Director of Surgical Gastroenterology, Medicover Hospitals, MVP, Visakhapatnam, Andhra Pradesh, India.
4Consultant Surgical Gastroenterologist, Medicover Hospitals, MVP, Visakhapatnam, Andhra Pradesh, India.
*Corresponding Author : Vishnuvardhan DAK
Lead Consultant, Radiology and Interventional Radiology, Medicover Hospitals, MVP, Visakhapatnam, Andhra Pradesh, India.
Email: bavisettyvijayalakshmi2@gmail.com
Received : May 07, 2024
Accepted : May 22, 2024
Published : May 29, 2024
Archived : www.jcimcr.org
Copyright : © Vishnuvardhan DAK (2024).
Abstract
To propose minimally invasive percutaneous approach in the management of refractory rectal variceal bleed. Rectal varices are porto-systemic collaterals that arise as a complication of portal hypertension. Bleeding is less common from rectal varices than from esophageal varices, but it is potentially life-threatening. A 28-year-old male presented to the Emergency department with one episode of hematemesis, hematochezia and severe abdominal pain with history of Extra Hepatic Portal Venous Obstruction (EHPVO), portal hypertension, portal cavernoma, esophageal varices, rectal varices and underwent splenectomy. Sigmoidoscopy revealed actively bleeding rectal varices. CT abdominal angiogram revealed variceal formation in the rectum. With failed endoscopic sclerotherapy and inaccessible endovascular transhepatic, transplenic approaches for embolisation, we successfully performed CT guided percutaneous NBCA glue injection of rectal varices with immediate and complete cessation of rectal bleed.
Keywords: Refractory rectal variceal bleed; CT guided percutaneous glue injection.
Citation: Vishnuvardhan DAK, Lavanya P, Botcha S, Das BB, Sahu S. Radiologic case Ct guided percutaneous Nbca glue injection of rectal varices for refractory rectal variceal bleed as a bailout. J Clin Images Med Case Rep. 2024; 5(5): 3083.
Case summary
A 28-year-old man presented to the Emergency Department with one episode of hematemesis, hematochezia and severe abdominal pain. He was a diagnosed case of EHPVO, portal hypertension with portal cavernoma, esophageal varices, rectal varices, and underwent splenectomy. There was history of syncopal attacks, vomiting and malena. No history of hypertension or diabetes mellitus.
On admission, his vital signs were recorded as heart rate of 115 Bpm, BP of 90/60 mmHg, sp02 97%, per abdomen was soft and non-tender, digital rectal examination showed fresh blood. He had severe anemia (hemoglobin 5.6 g/dL) and thrombocytopenia (platelets 1.39 lakh/cubic mm), total bilirubin level of 2.0 mg/dl with deranged liver function tests and coagulation profile. UGIE revealed two small esophageal varices without evidence of active bleeding from upper Gl tract. Sigmoidoscopy revealed actively bleeding rectal varices. Endoscopic sclerotherapy was done with 3 ml of setrol injected into the varix showing nipple sign, which achieved temporary hemostasis.
Imaging findings
CT Abdominal angiogram revealed variceal formation in the anorectum (Figure 1a-f) with features of EHPVO seen as diffuse narrowing of main portal vein and right branch due to chronic portal vein thrombus with portal cavernoma and varices at peripancreatic, mesenteric and anorectal regions. Post splenectomy status and incidental note of fusi-saccular aneurysm of size 6 mm and saccular aneurysm of size 5 mm along the course of proximal and distal segments of splenic artery respectively. Patient was initially managed with nor-adrenaline infusions, blood transfusions along with supportive symptomatic management to correct coagulation profile and liver function tests. Endoscopic Injection Sclerotherapy (EIS) was attempted without success as patient bled again the next day.
In view of inaccessibility of main portal vein due to chronic portal vein thrombus and portal cavernoma, inaccessibility of splenic vein due to post splenectomy status, TIPS, Endovascular Trans-hepatic and Trans-splenic embolization approaches could not be attempted. Hence, based on cross sectional imaging, we performed CT guided percutaneous glue injection of rectal varices using 3 ml of 50% cyanoacrylate glue (N-butyl-cyanoacrylate mixed with lipiodal in equal concentrations) under local anesthesia. The glue was injected using a 22G spinal needle into the right pararectal and rectal varices (Figure 2a-2d) at three levels under CT guidance with consequent obliteration of rectal varices leading to immediate and complete cessation of bleeding per rectum. Patient tolerated the procedure well.
Endoscopy performed after 1 week confirmed a marked shrinkage of rectal varices. CT abdominal angiogram performed 3 months (Figure 3a-3c) after the procedure revealed non-opacification of rectal varices. On 12 month follow up there was no recurrence of bleeding per rectum.
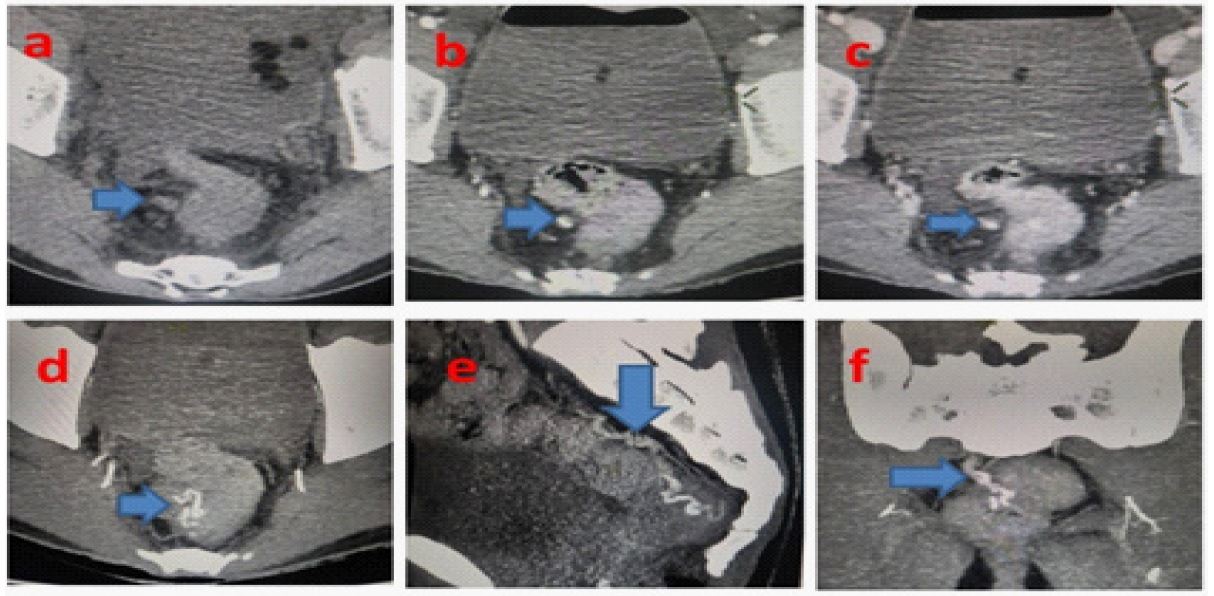
a: NECT of pelvis showing right pararectal collaterals, b: Collaterals in Arterial phase, C: Collaterals in Venous phase, d: Axial, e: Saggital, f: Coronal images showing the rectal varix filling from right pararectal bunch of interwined collaterals.
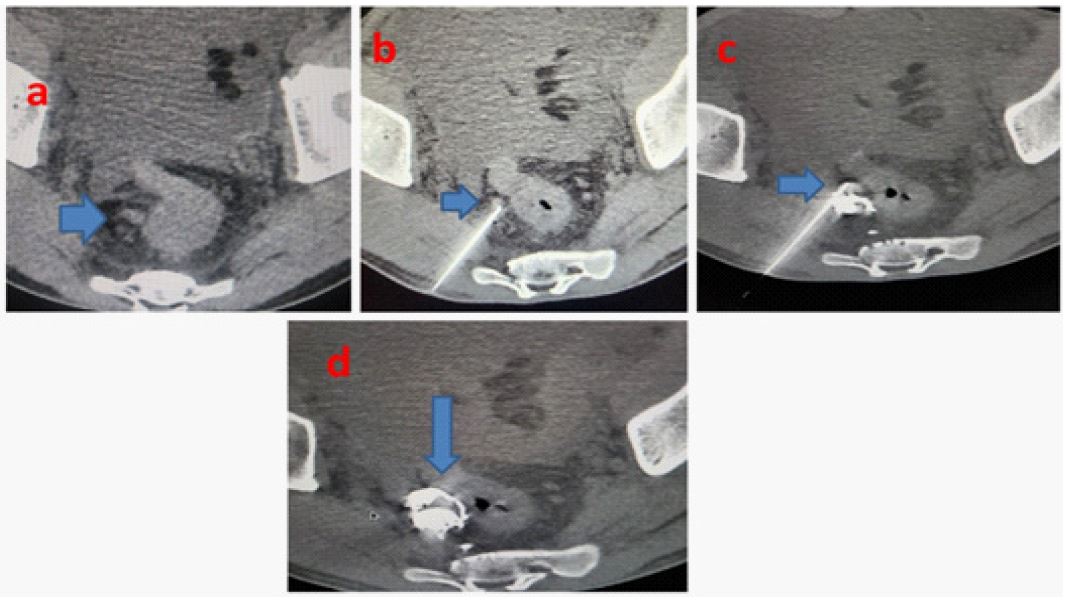
Axial NECT pelvis.
a: Showing right pararectal collateral, b: 22G LP needle tip in the collateral. C: Glue cast posteriorly ans 2nd level of glue injection into the collateral with needle tip in collateral anteriorly, d: Showing Final Glue Cast opacifying the rectal varix.
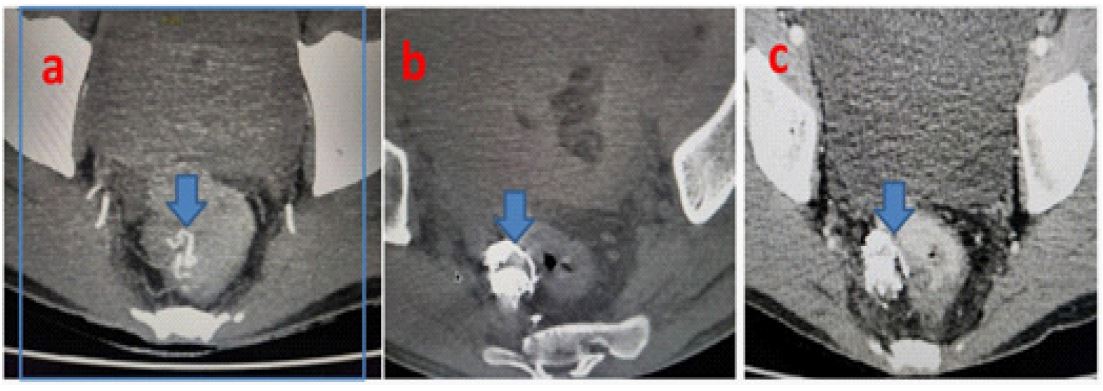
a: Pre-procedure axail CT angiogram of pelvis showing rectal varix (blue block arrow), b: Immediate post-procedure-axial CT pelvis showing glue cat in rectal varix (blue block arrow), c: 3 month post- procedure-axial CT angio pelvis showing glue cast nonopacifying rectal varix (blue block arrow).
Discussion
Anorectal varices represent porto-systemic collateral vessels that constitute a pathway for portal venous blood flow between the superior rectal veins of the inferior mesenteric system and the middle, inferior rectal veins of the iliac system. They manifest as dilated and engorged submucosal veins in the rectum. Anorectal varices most commonly result from portal hypertension secondary to cirrhosis. A variety of conditions that result in non-cirrhotic portal hypertension are also associated with the development of anorectal varices, including mesenteric or splenic vein obstruction from carcinoid syndrome or pancreatitis respectively, along with cavernous malformation of the portal vein [1]. Although rare, bleeding from rectal varices can be life threatening. The management of patients with rectal variceal bleeding is not well established. It is important to ensure hemodynamic stability with blood transfusion and to correct any coagulopathy prior to treating the bleeding varices. A variety of treatment modalities have successfully been employed to treat bleeding anorectal varices, including endoscopic therapies like Endoscopic Injection Sclerotherapy (EIS), Band Ligation (EBL) or Obturation (EVO). Interventional radiological procedures (Transjugular intrahepatic portosystemic shunt TIPS, endovascular transhepatic and transpslenic embolization of rectal varices), Surgical procedures (including simple suture ligation or stapled anopexy, mesenteric vein occlusion or porto-caval shunt surgery) [1].
In the current case scenario, with failed endoscopic sclerotherapy, TIPS and percutaneous transhepatic embolization were not possible due to the presence of portal vein thrombosis, portal cavernoma and complex bunch of anorectal variceal formation. Transplenic embolization was not possible owing to splenectomy.
After reviewing the CT Abdominal Angiogram, the right pararectal/anorectal varices (Figure 1a-f) were seen as bunch of intertwined collaterals coursing down from the plexus of veins in the pancreatic bed and nonvisualisation of inferior mesenteric vein, we planned and successfully performed glue obliteration of the rectal varices by direct puncture access with 22G spinal needle into the right pararectal varices, via the right transgluteal approach under CT guidance (Figure 2a-2d) and (Figure 3a-3c).
Similar case was described before where the procedure was performed using a hybrid Interventional Radiography/Computed Tomography (IVR-CT) system. In this case the right superior rectal vein was punctured with an 18 gauge needle under CT fluoroscopic guidance. Subsequently, a 0.035-inch guidewire (Radiofocus, Terumo, Tokyo, Japan) was inserted toward the feeding route of the varices and a 5F sheath introducer (Super Sheath, Medikit, Tokyo, Japan) was placed at the right superior rectal vein under fluoroscopic guidance followed by embolization of bilateral superior rectal veins using a steerable catheter 2. Comparatively, in our case there were right pararectal bunch of intertwined collaterals which couldn’t be cannulated owing to small size. Hence, introduction of sheath, micro catheter, DSA was not possible during embolization and entire procedure was performed successfully under CT guidance only.
Limitations like failure to inject glue into the anorectal varix, inadvertent injury to the rectal wall, pelvic hematoma; pelvic abcess formation should be considered while performing CT guided percutaneous glue injection of the rectal varices.
Conclusion
Navigating the intricate anatomy of extrahepatic portal venous obstruction, our experience of managing severe rectal variceal bleeding unveils a profound lesson. We believe that optimal utilisation of CT guided percutaneous glue injection technique can achieve timely resolution and should be considered in the management of such patients with refractory rectal variceal bleed. To the best of our knowledge, this novel approach hasn’t been described before in the literature.
References
- Robertson, M, Thompson AI, Hayes P. The management of bleeding from anorectal varices, Current Hepatology Reports. 2017; 16(4): 406-415. https://doi.org/10.1007/s11901-017-0382-6.
- Chatani S, Seki K, Sonoda A, Murakami Y, Tomozawa Y, et al. Bleeding anorectal varices treated by a direct puncture approach through the greater sciatic foramen: The utility of a steerable microcatheter for reverse catheterization. Radiol Case Rep. 2022; 17(4): 1104-1109. doi: 10.1016/j.radcr.2022.01.051.