
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Invasive pulmonary aspergillosis and lung abscess: Treatment lasting a total of 24 weeks
Samet Samanci*; Coşkun Doğan
Department of Chest Diseases, Faculty of Medicine, Istanbul Medeniyet University, Istanbul, Turkey.
*Corresponding Author : Samet Samanci
Department of Chest Diseases, Faculty of Medicine, Istanbul Medeniyet University, Istanbul, Turkey.
Tel: 555-857-15-75;
Email: drsametsamanci@gmail.com
Received : May 07, 2024
Accepted : May 23, 2024
Published : May 30, 2024
Archived : www.jcimcr.org
Copyright : © Samanci S (2024).
Abstract
A 75-year-old woman presented with complaints of cough, sputum, shortness of breath, and back pain. He was using Methylpredinosolone and Leflunomide due to his known diagnosis of Rheumatoid Arthritis. Fiberoptic Bronchoscopy was performed upon the presence of a cavitary lesion on thorax computed tomography. Antifungal treatment was started upon Aspergillus Terreus growth in bronchoalveolar lavage. She re-applied to the outpatient clinic at the 11th week of the treatment with the complaints of fever, cough, hemoptysis mixed with sputum. Ultrasonography-guided Trans Thoracic Needle Aspiration Biopsy was performed on the case. The case, which resulted in lung abscess as a result of pathology, was treated with amoxicillin-clavulonate tb. 2x1 g/day and metronidazole tb. 2 x 500 mg/day was started. Approximately 4 cm air cyst was seen in the control thorax CT of the patient whose complaints improved.
Citation: Samanci S, Doğan C. Invasive pulmonary aspergillosis and lung abscess: Treatment lasting a total of 24 weeks. J Clin Images Med Case Rep. 2024; 5(5): 3084
Introduction
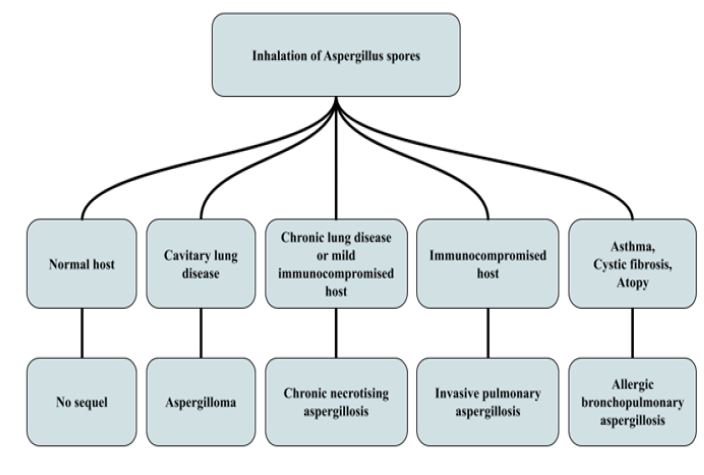
Aspergillus species, which are saprophytic in nature and whose spores can be found everywhere, are a mold fungus that can cause life-threatening lung disease with high morbidity and mortality, especially in immunocompromised cases. Invasive Pulmonary Aspergillosis (IPA), Chronic Necrotizing Aspergillosis, Allergic Bronchopulmonary Aspergillosis (ABPA) and Aspergilloma are the most common forms [1]. IPA usually develops only in severely immunocompromised cases. Against mold fungi [1]. Neutrophils (with roles such as Phagocytosis, oxidative burst, neutrophil extracellular traps) have an important role in step defense. In the second-line defense, normal host response is demonstrated by interferon, IL-2 and IL-12 stimulation through T-helper cell TH1, and IL-4 and IL-10 stimulation through TH2. IPA, which is an aggressive disease, occurs due to the invasion of the bronchial wall and arterioles of aspergillus hyphi that reach the lower respiratory tract by inhalation of spores in the host, which usually has a risk factor / immunosuppressive status (Figure 1). Clinically, fever, cough, sputum, shortness of breath, chest pain, and hemoptysis similar to pneumonia are among the common symptoms [2,3]. Although the symptoms are not specific to the disease, in thorax Computed Tomography (CT), lesions with central ground-glass opacity surrounded by a consolidation ring are called “reverse halo sign”. In invasive fungal infections, the reverse halo sign has been shown as an early sign caused by pulmonary infarction [4].
Lung Abscesses (AA) were a serious disease that could cause the death of approximately 75% of the cases in the absence of antibiotic treatment. Today, mortality can be high even with antibiotic and drainage treatment methods. Studies show that it may take 3-20 weeks to improve AA with antibiotic treatment, and the mortality rate of lung abscesses varies between 1% and 20% [5].
In this article; a case suspected of IPA with the appearance of radiological reverse halo sign while being followed up and treated with pneumonia symptoms and diagnosed with IPA with advanced examinations is presented. After IPA treatment, AP developed and was treated. Since it is a disease that can be cured with long-term treatment in both diseases, it is also presented as it is a rare condition that IPA is complicated with AA.
Case report
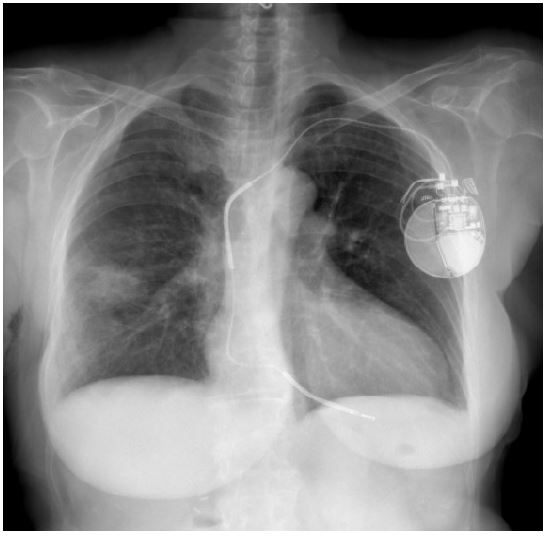
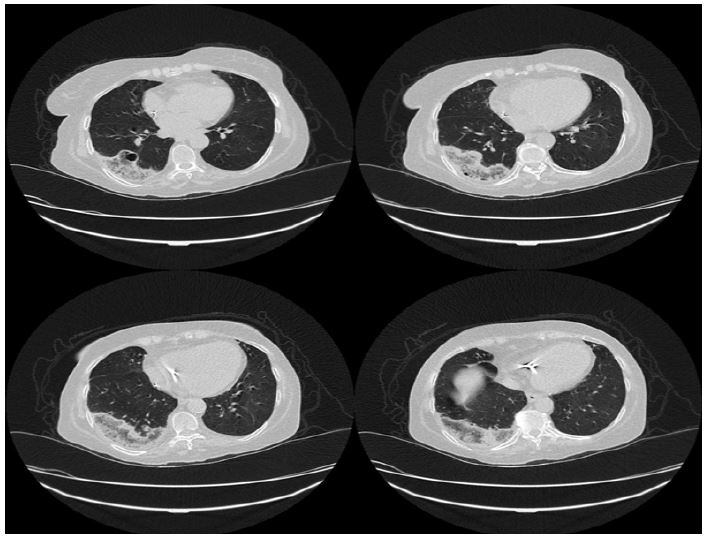
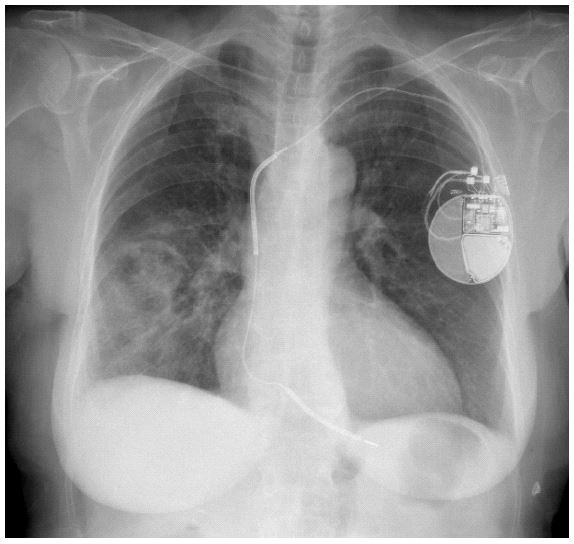
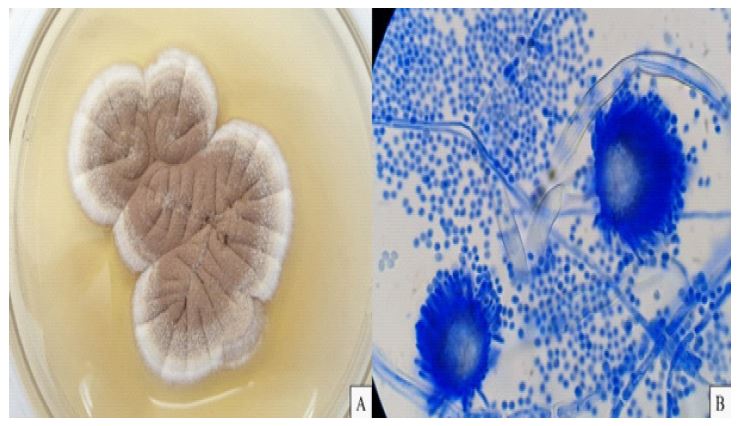
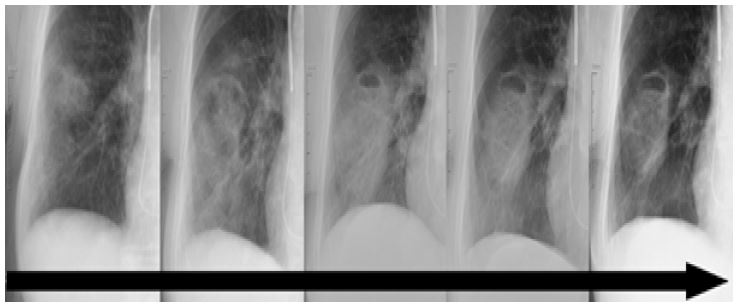
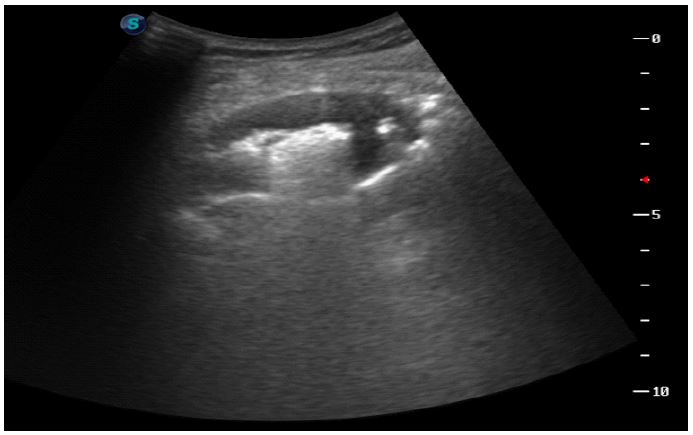
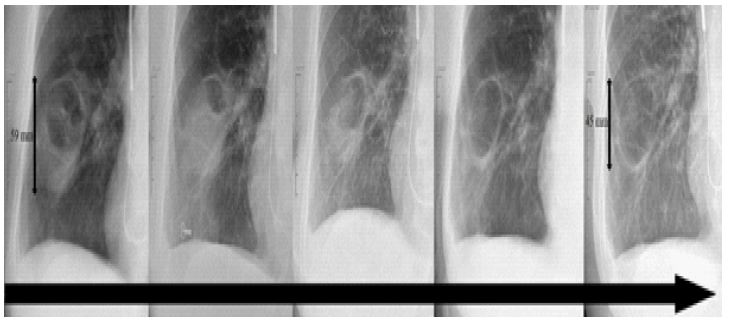
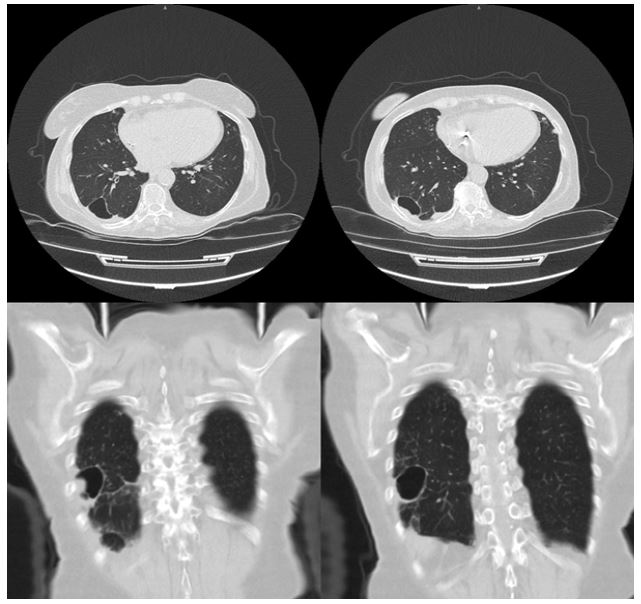
The history of a 75-year-old woman who presented with complaints of cough, sputum, shortness of breath, and back pain had a diagnosis of pacemaker (ICD), Hypertension, Diabetes Mellitus, and Rheumatoid Arthritis (RA) due to Chronic Heart Failure (CHF). He had been using Methylprednisolone 2 mg/day and Leflunomide 20 mg/day for 3 years due to RA. Her family history was unremarkable. She had no history of smoking. In the physical examination (FM), rale was heard in the middle and lower zone of the right lung with auscultation. In the Posterior-Anterior (PA) chest radiography (AG) of the case, irregularly bounded non-homogeneous density increase was observed in the right middle and lower zone (Figure 2). Thorax Computed Tomography (CT); approximately 101 x 49 mm in size in the posterobasal segment of the lower lobe of the right lung was reported as an increase in density suggesting an inverted halo appearance observed in the more dense consolidated central ground glass density in the periphery (Figure 3). Laboratory tests; Hemoglobin: 8.3 g/dL, Hematocrit: 26%, Platelet: 257.000/uL, White blood cell (WBC): 7200/uL, Procalcitonin: 0.125 μg/L, CRP: 97.6 mg/L, Urea: 30 mg/dL, Creatinine: 1.06 mg/dL, AST: 26 U/L, ALT: 21 U/L, LDH: 411 U/L, Na: 141 mmol/L, K: 4.2 mmol/L, Cl: 105 mmol/L, Ca: 9.1 mg/dL. Progression was observed in control PA AG and CRP: 242.98 mg/L, Procalcitonin: 2.2 μg/L in the 1st week of the started meropenem 3 x 1 g/day, teicoplanin 1 x 400 mg/day, clarithromycin 2 x 500 g/day empirical antibiotherapy treatment (Figure 4). Fiberoptic Bronchoscopy (FOB) was performed to send culture in Bronchoalveolar Lavage (BAL) to the patient. In Bal taken with fob, Galactomannan (GM) antigen optical density index was found to be positive as 2.579 (GM antigen >0.7). In addition, Aspergillus Terreus growth (Figure 5) was reported. The patient was given antifungal Voriconazole IV 2 x 400 mg/day loading dose and 2 x 200 mg/day maintenance treatment. Our case, who responded to the treatment clinically and radiologically, was planned to receive treatment with oral Vorikazanol tablet (tb) 2x200 mg/day for 6-12 weeks, was discharged and was followed up in the outpatient clinic. It was decided to complete the treatment of the case with slow regression in the control AG at 6 weeks of antifungal treatment to 12 weeks (Figure 6), she was re-interned to the chest diseases clinic due to the complaints of fever, cough, hemoptysis mixed with sputum during the outpatient clinic follow-ups. In the laboratory tests of the patient, White Blood Cell (WBC): 16500/uL, Procalcitonin: 0.831 μg/L, CRP: 358 mg/L of acute phase reactants. The patient was given ampicillin-sulbactam 2 x 2 g/day IV treatment for 7 days. No clinical radiological improvement was observed with antibiotherapy. Thoracic Ultrasonography (USG)-guided Trans Thoracic Needle Aspiration Biopsy (TTIAB) and Tru-cut Biopsy were performed on the cavitary lesion with a sonographically hyperechogenic thick wall structure of approximately 6 x 4 cm in size peripherally in the right hemithorax and necrotic-air bronchograms were observed in the middle (Figure 7). As a result of the pathology, histocytomorphological findings were reported to be compatible with the abscess wall. ARB was negative from TTİAB material, there was no growth in the fungal culture, non-specific culture and tuberculosis culture sent. Since the general condition is good and the clinic is stable, oral amoxicillin-clavulonate tb. 2x1 g/day and metronidazole tb. 2 x 500 mg/day treatment was arranged and he was followed up in the outpatient clinic. In the follow-ups after antibiotherapy, the complaints of fever, cough, hemoptysis mixed with sputum decreased. Regression was observed in PA AGs taken in the monthly follow-up of the patient who received antibiotic treatment for 12 weeks (Figure 8). On control thorax CT, an air cyst with a diameter of 4 cm was observed in the superior segment of the lower lobe of the right lung (Figure 9).
Discussion
IPA and AP, which are two diseases with high mortality and morbidity and may require the longest treatment period after tuberculosis, are rare. In this article, a very long-term treatment process of an immunosuppressive case who regained his health with careful and patient follow-up of both the following doctor and the patient receiving treatment is shared.
Acute myeloid leukemias and myelodysplastic syndromes, other hematological malignancies (acute lymphoblastic leukemias, multiple myeloma..), allogeneic hematopoietic stem cell transplant cases, chimeric antigen receptor T-Cell therapy cases, acquired or inherited immunodeficiency, solid organ transplantations, solid tumor cases, critically patients in intensive care units, viral pneumonia cases and cases with the diagnosis of inflammatory and autoimmune diseases such as RA are the cases with risk factors for IPA [6]. Today, as in most diseases, the increase in diagnosis and treatment opportunities in RA patients leads to a prolonged life expectancy and an increase in the number of patients receiving immunosuppressive treatment. For this reason, it is an undeniable fact that there is an increase in the number of lung infections caused by opportunistic pathogens in cases receiving immunosuppressive treatment, especially RA [7]. Two of the main drugs used in the treatment of RA are antirheumatic and glucocorticoid drugs. While antirheumatic drugs may be useful in suppressing the hyperactive immune system seen in RA patients, they also have the possibility to increase the risk of serious lung infection due to reasons such as suppressing the glycosylation of adhesion molecules, suppressing immunosuppressive and nuclear factor kappa activation [8]. In addition, while glucocorticoids affect the inflammatory cascade of the disease, such as the inhibition of the proliferation of macrophages and fibroblasts, they also play a role in Interleukin-1 (IL-1), IL6, tumor necrosis factor alpha blockade. Therefore, glucocorticoids are also associated with serious side effects such as increased risk of infection [9,10]. In a meta-analysis study in which Elsouri KN et al. [11] included a total of 125 research articles, it was observed that patients under antirheumatic and glucocorticoid combination therapy were more likely to develop lung infection than the use of antirheumatic therapy alone in RA. Studies have shown that causes such as disease and drug use that cause immunosuppression are among the biggest risk factors for Aspergillus [2,12]. In our case, he had been using Methylprednisolone and Leflunomide for 3 years due to RA.
Lung abscess and IPA have similar risk factors. Causes such as hematological or solid organ tumors, transplant patients, HIV infection and chronic corticosteroid use constitute risk factors in AA [13]. When the English literature was examined, a case of Shu ÇC et al. [14] regarding the development of AA after IPA was found. In this case report, an AA due to Clostridium Baratii was reported in a 47-year-old male patient with Invasive Pulmonary Aspergillosis. In this presentation, the authors emphasized that the tendency of Aspergillus species to invade hyphae blood vessels, which leads to local thrombosis and tissue infarction, may contribute to the formation of lung abscess. Unfortunately, the factor that may lead to AA could not be produced in our case report. The material taken by thoracic USG was examined pathologically, and there was no growth in fungal culture and non-specific culture. The reason for this is that, as Bartlett JG et al. [15] stated, the increased broad-spectrum empirical antibiotic treatment before the bacteriological study especially affected anaerobic bacteria may explain this difference.
In our case, we applied voriconazole for 12 weeks as an antifungal treatment due to IPA. In the 2016 update of the Infectious Diseases Society of America, Patterson et al. also strongly recommend voriconazole as the primary treatment in the treatment of IPA, with a high level of evidence. In addition, 6-12 weeks of treatment is recommended in the same guide [1]. In the follow-up of our patient, since the lesion in the lung was complicated and he was diagnosed with AA, our patient was given antibiotic treatment for 12 weeks and followed up until clinical radiological recovery. Since there is no full consensus on the duration of AA treatment, it is recommended that the decision should be made according to the clinic and radiology of the case. Some studies have shown that antibiotic treatment of lung abscess may take 3-20 weeks [16,17].
In conclusion, different infectious agents of the lung may be effective in cases receiving immunosuppressive treatment. Especially in diseases such as IPA and AA, radiological recovery may be late and treatment may take a long time in these cases.
Declarations
Funding: I and my spouse/partner have had no relevant financial interests or personal affiliation.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest: None declared.
Artificial intelligence: Generative Artificial Intelligence (AI) and artificial intelligence- assisted technologies were not used during the writing of this article.
Submission declaration and verification: This submission has not been published previously and not under consideration for publication Manuscript has been ‘spell checked’ and ‘grammar checked’.
References
- Patterson TF, Thompson GR, Denning DW, Fishman JA, Hadley S, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 63(4): e1-e60.
- Kousha M, Tadi R, Soubani AO. Pulmonary aspergillosis: a clinical review. Eur Respir Rev. 2011; 20(121): 156-74.
- Albelda SM, Talbot GH, Gerson SL, Miller WT, Cassileth PA. Pulmonary cavitation and massive hemoptysis in invasive pulmonary aspergillosis. Influence of bone marrow recovery in patients with acute leukemia. Am Rev Respir Dis. 1985; 131(1): 115-20.
- Godoy MC, Viswanathan C, Marchiori E, Truong MT, Benveniste MF, et al. The reversed halo sign: Update and differential diagnosis. Br J Radiol. 2012; 85(1017): 1226-35.
- Maitre T, Ok V, Calin R, Lassel L, Canestri A, et al. Pyogenic lung abscess in an infectious disease unit: A 20-year retrospective study. Ther Adv Respir Dis. 2021; 15: 17534666211003012.
- Ledoux MP, Herbrecht R. Invasive Pulmonary Aspergillosis. J Fungi (Basel). 2023; 9(2): 131.
- McNeil MM, Nash SL, Hajjeh RA, Phelan MA, Conn LA, et al. Trends in mortality due to invasive mycotic diseases in the United States, 1980-1997. Clin Infect Dis. 2001; 33(5): 641-7.
- Ulusoy H, Bilgici A, Kuru O, Celenk C. Pulmonary abscess due to leflunomide use in rheumatoid arthritis: a case report. Rheumatol Int. 2005; 25(2): 139-42.
- Mori S, Ueki Y, Miyamura T, Ishii K, Hidaka T, et al. Outcomes and risk factors for mortality in Pneumocystis pneumonia patients with rheumatoid arthritis: A multicentre retrospective cohort study. Mod Rheumatol. 2023: 4; 33(4): 723-31.
- George, Hsu JY, Hennessy S, Chen L, Xie F, et al. Risk of serious infection with low-dose glucocorticoids in patients with rheumatoid arthritis: an instrumental variable analysis. Epidemiology. 2022; 33: 65-74.
- Elsouri KN, Arboleda V, Basbous L, Heiser S, Collins DP, et al. Glucocorticoid use in rheumatoid arthritis patients and the onset of pneumonia: A systematic review and meta-analysis. J Osteopath Med. 2023; 123(4): 179-186.
- Hung ML, Liao HT, Chen WS, Chen MH, Lai CC, et al. Invasive aspergillosis in patients with systemic lupus erythematosus: A retrospective study on clinical characteristics and risk factors for mortality. Lupus. 2018; 27(12): 1944-1952.
- Mansharamani N, Balachandran D, Delaney D, Zibrak JD, Silvestri RC, et al. Lung abscess in adults: clinical comparison of immunocompromised to non-immunocompromised patients. Respir Med. 2002; 96(3): 178-85.
- Shu CC, Yao M, Hung CC, Ku SC, Yu CJ, et al. Lung abscess due to Clostridium baratii infection in a patient with invasive pulmonary aspergillosis. J Clin Microbiol. 2008; 46(3): 1153-4.
- Bartlett JG. The role of anaerobic bacteria in lung abscess. Clin Infect Dis. 2005; 40(7): 923-5.
- Takayanagi N, Kagiyama N, Ishiguro T, Tokunaga D, Sugita Y. Etiology and outcome of community-acquired lung abscess. Respiration. 2010; 80(2): 98-105.
- Kuhajda I, Zarogoulidis K, Tsirgogianni K, Tsavlis D, Kioumis I, et al. Lung abscess-etiology, diagnostic and treatment options. Ann Transl Med. 2015; 3(13): 183.