
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
A particular dermoscopic clue of lichen pigmentosus in a patient with corticotropin deficiency
Meryem Soughi1*; Oumaima Bouraqqadi2; Zakia Douhi1; Sara Elloudi1; Hanane Baybay1; Fatima Zahra Mernissi1
1Dermatology Department, University Hospital Hassan II, URL CNRST N15; Human Pathology, Biomedicine and Environment Laboratory, Faculty of Medicine, Pharmacy and Dental Medicine of Fez, Sidi Mohamed Ben Abdellah University, Fez, Morocco.
2Dermatology Department, Faculty of Medicine, Pharmacy and Dental Medicine, University Hospital Hassan II Fez, Morocco.
*Corresponding Author : Meryem Soughi
Dermatology Department, University Hospital Hassan II, URL CNRST N15; Human Pathology, Biomedicine and Environment Laboratory, Faculty of Medicine, Pharmacy and Dental Medicine of Fez, Sidi Mohamed Ben Abdellah University, Fez, Morocco.
Email: msoughi@gmail.com
Received : May 06, 2024
Accepted : May 23, 2024
Published : May 30, 2024
Archived : www.jcimcr.org
Copyright : © Soughi M (2024).
Abstract
Our article reports a particular dermoscopic clue in the perioral area of a patient with corticotropin deficiency. The contribution of dermoscopy was crucial in that we could suggest melanoderma with here Addison’s disease. Still, the presence of a particular aspect of annular peri follicular pigmentation defining circles led us to perform a biopsy which confirmed the diagnosis of lichen pigmentosus. These dermoscopic appearance-defined pigmented circles correlated well with the histology, which showed severe peripilar pigment incontinence associated with a lichenoid reaction.
Keywords: Lichen pigmentosus; Dermoscopy; Fibrotic frontal alopecia.
Citation: Soughi M, Bouraqqadi O, Douhi Z, Elloudi S, Baybay H, et al. A particular dermoscopic clue of lichen pigmentosus in a patient with corticotropin deficiency. J Clin Images Med Case Rep. 2024; 5(5): 3086.
Introduction
Lichen Planus Pigmentosus (LPP) is a pigmentary disorder that manifests as brown to grey-brown macules and patches mainly on the face, neck, and intertriginous areas, particularly prevalent in individuals with dark skin [1].
We report a particular clinical and dermoscopic presentation in a patient with corticotropin deficiency.
Case presentation
A 52-year-old female patient, phototype IV, with a history of asthma, steroid diabetes, and corticotropin deficiency, presented with multiple ill-defined pigmented macules on the cheeks and forehead, we also found a pigmentation along the palmar furrows, possibly associated with her corticotropin deficiency. Dermoscopy revealed a homogeneous pseudo-network on the temporal and malar areas, and perifollicular annular pigmentation on the perioral area without hair loss (Figures 1a, 1b). Given this distinct presentation, a skin biopsy at the peribuccal area was performed confirming the diagnosis of lichen pigmentosus (Figure 1b). The patient was successfully treated with topical retinoid.
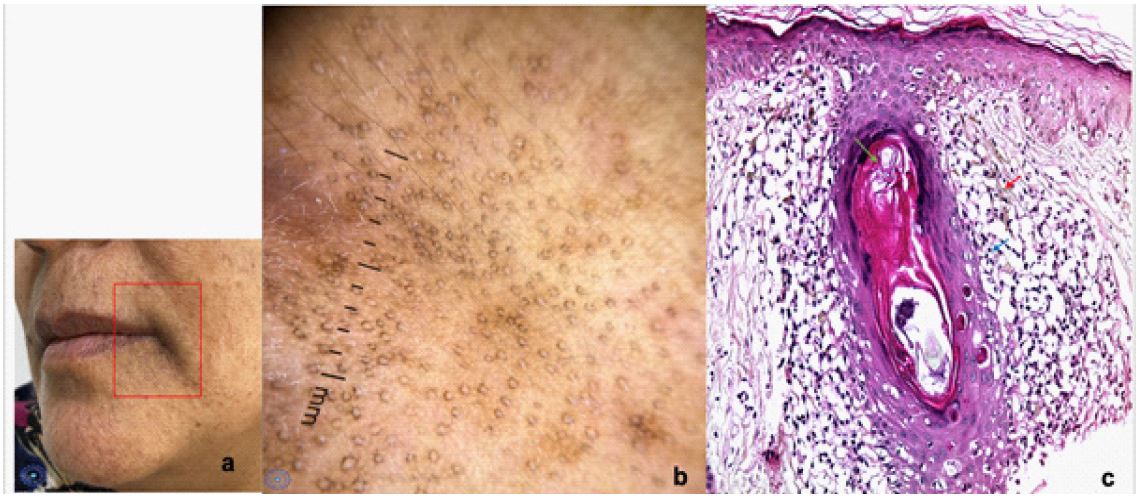
1b: Annular pigmented pattern on dermoscopy.
1c: Coloration (HES G x 200) Basal vacuolation, hair sheaths affected by a lichenoid infiltrate with of small lymphocyte (blue arrow), keratotic pilar plug (green arrow), peripilar pigmentary incontinence (red arrow).
Discussion
Dermoscopic features of lichen pigmentosus reported in the literature include a brown pseudonetwork, dots, and globules in various patterns that represent varying degrees of pigment incontinence, along with telangiectasias and reduced vellus hair density [1]. However, our case exhibited a distinct feature: A well-defined perifollicular circle devoid of interfollicular skin involvement, along with palmar folds pigmentation linked probably to her corticotropin deficiency, hence the diagnostic ambiguity. Histopathologically, these circles can be explained by notable peripilar pigmentary incontinence which it associated to lichenoid infiltrate, contrasting with preserved facial hair and the absence of Fibrotic Frontal Alopecia (FFA). This contradicts the findings by Pirmez et al. where LPP was considered a herald sign of FFA [2]. Therfore, vigilant scalp and hairline examination for early FFA indicators in each consultation are crucial for optimal management.
Conclusion
The purpose of presenting this case is to highlight this particular aspect of lichen pigmentosus and to recommend the use of a dermoscope in the presence of any pigmentation, to help the dermatologist make an accurate diagnosis without the need for a biopsy.
Source(s) of support: None.
Conflicting interest: None.
References
- Krueger L, Saizan A, Stein JA, Elbuluk N. Dermoscopy of acquired pigmentary disorders: A comprehensive review. Int J Dermatol. 2022; 61(1): 7-19. doi:10.1111/IJD.15741.
- Pirmez R, Duque-Estrada B, Donati A, et al. Clinical and dermoscopic features of lichen planus pigmentosus in 37 patients with frontal fibrosing alopecia. British Journal of Dermatology. 2016; 175(6): 1387-1390. doi:10.1111/BJD.14722.