
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
The crossing duct sign of pancreas divisum
Sara Essetti*; Kaoutar Imrani; Chaymae Faraj; Sara Ez-Zaky; Nabil Moatassim Billah; Itimad Nassar
Central Radiology Department, Ibn Sina University Hospital Center, Mohammed V University, Rabat, Morocco.
*Corresponding Author : Sara Essetti
Central Radiology Department, Ibn Sina University Hospital Center, Mohammed V University, Rabat, Morocco.
Email: s.essetti@gmail.com
Received : May 08, 2024
Accepted : May 24, 2024
Published : May 31, 2024
Archived : www.jcimcr.org
Copyright : © Essetti S (2024).
Citation: Essetti S, Imrani K, Faraj C, Ez-Zaky S, Billah NM, et al. The crossing duct sign of pancreas divisum. J Clin Images Med Case Rep. 2024; 5(5): 3088.
Description
Pancreas divisum is the most common congenital malformation of the pancreatic ductal system, it has been reported to affect approximately 4-14% of the general population [1].
It results from failure of fusion of dorsal and ventral pancreatic duct during the early weeks of embryonic life (6-8 weeks). As a result, the dorsal duct (Santorini duct) drains most of the pancreatic parenchyma through the minor papilla, whereas the ventral duct (duct of Wirsung) drains a portion of the pancreatic head and uncinate process, through the major papilla [2].
Most patients with pancreas divisum are asymptomatic; however, it has been considered as a predisposing factor for chronic abdominal pain and recurrent idiopathic pancreatitis [3].
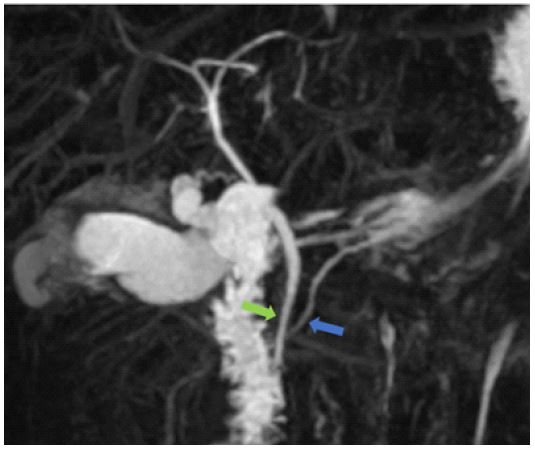
Magnetic Resonance Cholangiopancreatography (MRCP) is the modality of choice for diagnosis. It shows the typical crossing duct sign (Figure 1) which refers to the joining of the main pancreatic duct (dorsal) into the accessory papilla, crossing over the Common Bile Duct (CBD), which joins with the ventral pancreatic duct into the duodenum at the major papilla.
The treatment of pancreas divisum is typically reserved for symptomatic patients [4]. Endoscopic sphincterotomy is considered the first-line treatment.
References
- Kim HJ, Kim MH, Lee SK, Seo DW, KimYT, Lee DK et al. Normal structure, variations, and anomalies of the pancreaticobiliary ducts of Koreans: a nationwide cooperative prospective study. Gast rointest Endosc 2002;55:889-96.
- Guirat, A., Abid, M., Amar, M. B., Rebai, W., & Beyrouti, M. I. (2009). Pancréas divisum. La Presse Médicale, 38(9), 1353–1359. doi:10.1016/j.lpm.2008.05.024.
- Mortelé K, Rocha T, Streeter J, Taylor A. Multimodality Imaging of Pancreatic and Biliary Congenital Anomalies. Radiographics. 2006;26(3):715-31. doi:10.1148/rg.263055164.
- Morgan D, Logan K, Baron T, Koehler R, Smith J. Pancreas Divisum: Implications for Diagnostic and Therapeutic Pancreatography. AJR Am J Roentgenol. 1999;173(1):193-8. doi:10.2214/ajr.173.1.10397125.