
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Coronary endarterectomy and long stent removal of left anterior descending artery in a patient with in-stent restenosis
Mohammed Tribak1*; Christ-Marion Adanho1; Yassine Elmourabit1; Lalla Hasna Leghlimi2; Aida soufiani3; Zineb Agoumy3; Samah El-Mhadi3; Lahcen Marmade1; Said Moughil1
1Department of Cardiovascular Surgery “B”, Ibn Sina University Hospital, Mohamed V University, Rabat, Morocco.
2Department of Cardiovascular Anesthesia” B”, Ibn Sina University Hospital, Mohamed V University, Rabat, Morocco.
3Department of Cardiology “A”, Ibn Sina University Hospital, Mohamed V University, Rabat, Morocco.
*Corresponding Author : Mohammed Tribak
Department of Cardiovascular Surgery “B”, Ibn Sina University Hospital, Mohamed V University, Rabat, Morocco.
Tel: +212667662898;
Email: tribakmed@yahoo.fr
Received : May 07, 2024
Accepted : May 27, 2024
Published : Jun 03, 2024
Archived : www.jcimcr.org
Copyright : © Tribak M (2024).
Abstract
Coronary endarterectomy constitutes a valid surgical option when complete revascularization is threatened due to in stent restenosis involving diffuse target vessel disease. Despite its promising potential for complete revascularization in diffuse coronary artery disease, its safety and effectiveness are still doubted due to increased mortality and perioperative myocardial infarction rates. Diffuse coronary artery disease affecting side branches, severe calcification of coronary arteries and in-stent restenosis following full-metal jacket procedures are its indications. We present a case of a 67-years old women with in-stent restenosis of distal left anterior descending artery and diffusely disease distal left anterior descending artery. We describe our surgical management and a review of literature.
Keywords: Coronary endarterectomy; In-stent restenosis; Diffuse coronay artery disease; Left anterior descending artery.
Citation: Tribak M, Adanho CM, Elmourabit Y, Leghlimi LH, Soufiani A, et al. Coronary endarterectomy and long stent removal of left anterior descending artery in a patient with in-stent restenosis. J Clin Images Med Case Rep. 2024; 5(6): 3091.
Introduction
In-Stent Restenosis (ISR) remains a major complication of Percutaneous Coronary Intervention (PCI), even in the current era of Full-Metal Jacket (FMJ) [1]. Optimal management of ISR is still controversial, Coronary Artery Bypass Grafting (CABG) provides better outcomes in patients with ISR [2]. However, CABG may fail in terms of complete revascularization when the side branches are involved in and affected by long-segment ISR. Coronary Endarterectomy (CE) is the removal of coronary atherosclerotic core through an arteriotomy. In its initial stages, CE was considered technically difficult with high operative mortality and perioperative Myocardial Infarction (MI) rates but this technique has been revived recently with reports stated the safety, efficacy and favorable long-term outcomes [3]. We present a case of a 67-years old women with ISR of distal LAD and diffusely disease distal LAD with postinfarction ventricular septal defect who underwent CE and FMJ-LAD distally removal, LAD repair by on-lay saphenous vein patch with LITA-LAD grafting and repair of ventricular septal defect.
Case presentation
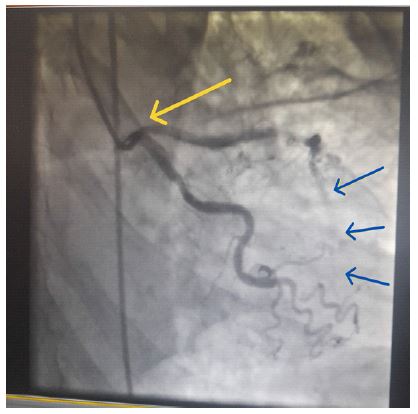
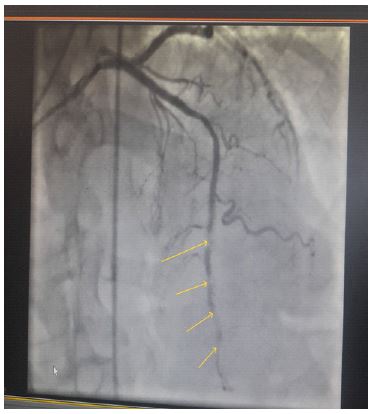
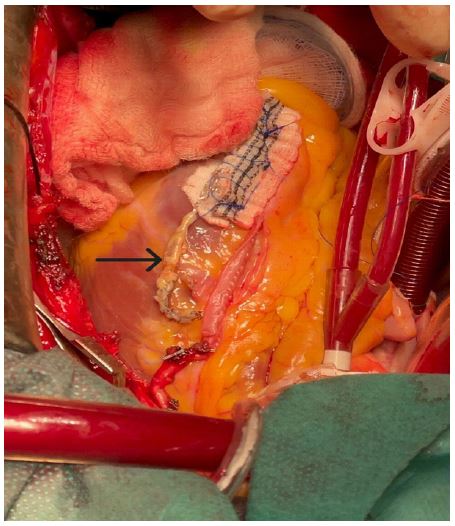
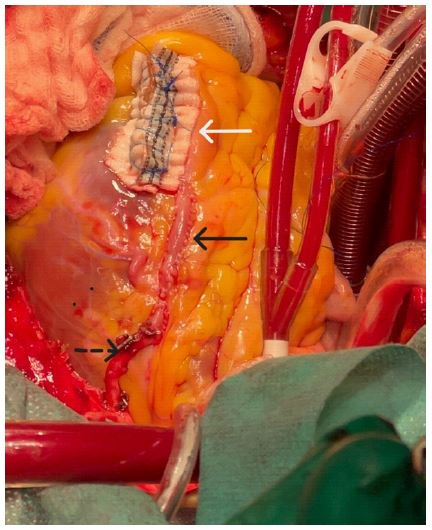
A 67-year-old women, with cardiovascular risk factors of age, hypertension, type 2 diabetes, dyslipidemia and menopause. She is followed for coronary artery disease since 2016 related to a single-vessel disease of proximal LAD which was treated with a FMJ procedures. One year later, due to onset of acute chest pain, a coronary angiography revealed single-vessel disease of distal LAD which was treated with a FMJ procedures (2.5 mm/16 mm), whereas the FMJ-LAD proximal was patent. Six years later, she was admitted for Non-ST-elevation myocardial infarction related to a FMJ-LAD distally occluded with a poor target vessel and ostial stenosis of LAD. Obtuse marginal artery and right coronary artery were atheromatous without significant lesion and the FMJ-LAD proximal was patent (Figures 1 and 2). FMJ procedures (2.5/30 mm) to the distal portion of the occluded stent showed no reflow in distal LAD and patient was referred to surgery. At admission, physical examination showed a blood pressure at 102/70 mmHg, a heart rate at 107 bpm, a systolic murmur at all auscultatory sites, in the form of a wheel spoke. Electrocardiography showed regular sinus rhythm at 108 cycles per minute, Q wave of necrosis and slight ST-segment elevation in antero-septo-apical leads. Transthoracic echocardiography revealed an apical muscular ventricular septal defect, measured 10 mm in diameter, shunting from left to right ventricle. A good left ventricular fonction. There were akinesia in the apical-septal segment and severe hypokinesia in the apex, in the others apical segments and in the median anteroseptal segment. She underwent CE with FMJ-LAD distally removal, longitudinal saphenous vein patch covering the arteriotomy (60 mm long), LITA-LAD grafting and repair of ventricular septal defect using prosthetic patch (Figures 3 and 4). The postoperative course was uneventful. Heparin infusion was initiated 6 hours after arrival in the intensive care unit. After 2 days, this was replaced by warfarin sodium and aspirin. Patient was discharged on dual antiplatelet therapy using aspirin, clopidogrel and warfarin continued for three months maintaining an international ratio of 2. Clopidogrel was continued one year postoperatively and aspirin was continued lifelong. The 3-months follow-up found the patient in good clinical condition, transthoracic echocardiography showed normal biventricular function with no residuel postoperative ventricular septal defect.
Discussion
ISR remains a major complication after PCI even in the current era of FMJs, and occurs in 3-20% of patients [1]. Repeat PCI is the most commonly used technique for the treatment of ISR, but the recurrence rate is very high and long-term outcomes are unsatisfactory [4]. Although CABG reportedly has better outcomes than PCI in patients with ISR [2]. CE was firstly described by Bailey and al in 1957 in diffusely diseased coronary arteries [5]. The importance of this technique is the possibility of complete myocardial revascularization as opposed to an otherwise incomplete revascularization by conventional CABG associated with a higher operative mortality, recurrent angina, perioperative and late MI, as well as higher reoperation rates [6]. Despite its promising potential for complete revascularization in diffuse Coronary Artery Disease (CAD), its safety and effectiveness are still doubted due to increased mortality and perioperative MI rates [7]. Endothelium destruction subsequent to CE may trigger acute thrombogenesis or embolization of atheromatous debris may occur, leading to a postoperative MI [8]. Endarterectomy of the stented artery is technically demanding. We performed a open endarterectomy, the whole procedure was performed under direct vision. A longitudinal arteriotomy (60 mm) of LAD beyond the limits of the stents was performed. En bloc long-segment stent and atheromatous plaques were completely removed from both the main vessel and the side branches. We performed a longitudinal saphenous vein patch covering the arteriotomy with a running suture so that the patch made up most of the reconstructed vessel and a subsequent LITA-LAD grafting. On-lay patch grafting using the ITA are the possible reconstruction approaches for bypass grafting [9].
Various regimens have been recommended. Aspirin alone protocol lags behind due to disturbed endothelial integrity in case of CE thus failing to achieve long-term graft patency [10]. Either heparin infusion followed by warfarin or double antiplatelet therapy (Clopidogrel stoped 12 months later) immediately after the operation are reasonable [11]. Heparin is withheld when an International Normalized Ratio (INR) between 2 and 3 is achieved followed by oral administration of warfarin 3 months postoperatively with permanent aspirin alone intake is recommended [12].
Conclusion
CE and stent removal is a safe and effective technique used in patients with ISR involving diffuse target vessel disease. CE should only be performed by highly experienced surgeons in a highly selected group of patients, when there is no other choice for achieving complete revascularization.
Declarations
Conflict of interest statement: The authors report no conflicts of interest.
Ethical approval: No approval is required.
Consent: The patient consented to her case to be published in the scientific literature.
References
- Dangas GD, Claessen BE, Caixeta A, Sanidas EA, Mintz GS, Mehran R. In-stent restenosis in the drug-eluting stent era. J Am Coll Cardiol. 2010; 56: 1897-907.
- Moustapha A, Assali AR, Sdringola S, Vaughn WK, Fish RD, Rosales O et al. Percutaneous and surgical interventions for in-stent restenosis: long-term outcomes and effect of diabetes mellitus. J Am Coll Cardiol. 2001; 37: 1877-82.
- Nemati MH, Astaneh B, Khosropanah S. Outcome and graft patency in coronary artery bypass grafting with coronary endarterectomy. Korean J Thorac Cardiovasc Surg. 2015; 48: 13-24.
- Kobayashi Y, De Gregorio J, Kobayashi N, Akiyama T, Reimers B, Finci L et al. Stented segment length as an independent predictor of restenosis. J Am Coll Cardiol. 1999; 34: 651-9.
- Bailey C.P, May A, Lemmon W.M. Survival after coronary endarterectomy in man. 1957; 164: 641-646.
- Soylu E, Harling L, Ashrafian H, Casula R, Kokotsakis J, Athanasiou T. Adjunct coronary endarterectomy increases myocardial infarction and early mortality after coronary artery bypass grafting: A meta-analysis. Interact. Cardiovasc. Thorac. Surg. 2014; 19: 462-473.
- Minale C, Nikol S, Zander M, et al. Controversial aspects of coronary endarterectomy. Ann Thorac Surg. 1989; 48: 235-41.
- Soylu E, Harling L, Ashrafian H, Athanasiou T. Should we consider off-pump coronary artery bypass grafting in patients undergoing coronary endarterectomy? Interact Cardiovasc Thorac Surg. 2014; 19: 295-301.
- Stavrou A, Gkiousias V, Kyprianou K, Dimitrakaki IA, Challoumas D, Dimitrakakis G. Coronary endarterectomy: the current state of knowledge. Atherosclerosis. 2016; 249: 88-98.
- Karavas AN, Gudbjartson T, et al. Left anterior descending coronary endarterectomy: early and late results in 196 consecutive patients. Ann Thorac Surg. 2004; 78: 867-73.
- Tiruvoipati R, Loubani M, Peek G. Coronary endarterectomy in the current era. Curr Opin Cardiol. 2005; 20: 517-20.
- Vafaey HR, Salehi Omran MT, Abbaspour S, Banihashem N, Faghanzadeh Ganji G. Anti-coagulation therapy following coronary endarterectomy in patient with coronary artery bypass graft. Caspian J Intern Med. 2018; 9: 27-31.