
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Heat’s mark: Unraveling erythema ab igne
Víctor García-Rodríguez1*; Albert Martin-Poch1; Sonia Romero-Romero1; Mariona Pintiado-Gàmez1; Maribel Fernández-Velasco1; Maribel Iglesias-Sancho1; Maite Fernández-Figueras2
1Dermatology Department, Sagrat Cor University Hospital, Quirónsalud Hospital Group, Barcelona, Spain.
2Pathology Department, General University Hospital of Catalonia, Sant Cugat del Vallés, Barcelona, Spain.
*Corresponding Author : Víctor García-Rodríguez
Department of Dermatology, Sagrat Cor University Hospital, Quirónsalud Hospital Group, Barcelona, Spain.
Tel: +34-93-3221111;
Email: derma.vgr@gmail.com
Received : May 08, 2024
Accepted : May 27, 2024
Published : Jun 03, 2024
Archived : www.jcimcr.org
Copyright : © García-Rodríguez V (2024).
Abstract
We report a case of a 76-year-old woman presenting with a long-standing asymptomatic erythematous-brownish reticular rash on the back and glutes. After thorough medical history and examination, the patient recognized she lived in a rural area and admitted to sitting with her back to the chimney for long periods of time. Erythema Ab Igne was suspected, and a biopsy was performed to rule out other conditions. We hope exposure to this paradigmatic clinical image may aid in the differential diagnosis of reticular rashes.
Keywords: Erythema Ab Igne; Clinical diagnosis; Dermatology; Pathology.
Abbreviations: EAI: Erythema Ab Igne.
Citation: García-Rodríguez V, Martin-Poch A, Romero-Romero S, Pintiado-Gàmez M, Fernández-Velasco M, et al. Heat’s mark: Unraveling erythema ab igne. J Clin Images Med Case Rep. 2024; 5(6): 3092.
Introduction
Erythema Ab Igne (EAI) is a long-known dermatological entity characterized by a reticular rash related to long-term heat exposure insufficient to cause burn. We present a clinico-pathological case of EAI. Follow-up is recommended in these patients owing to the presumable cutaneous malignancy which can appear thereon.
Case presentation
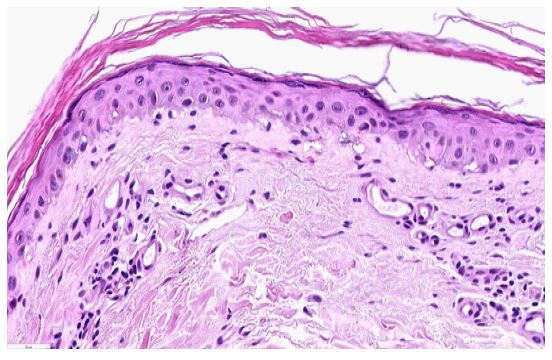
A 76-year-old woman presented an asymptomatic, erythematous-brownish reticular rash on the posterior aspect of the trunk, arms and glutes (Figure 1). After thorough medical inquiry, the patient admitted to sitting with her back to the chimney for long periods of time. Histopathology revealed prominent dermal angiogenesis, extravasation of red blood cells and mild perivascular lymphocytic infiltrate. The epidermis showed dysmaturative changes, focal vacuolar degeneration, and hyperkeratosis. These changes confirmed the diagnosis of EAI (Figure 2).

Discussion
EAI is allegedly caused by prolonged cumulative exposure to infrared radiation coming from heat sources, not reaching the threshold for burning [1]. EAI has long been recognized, especially in patients using stoves, and can manifest anywhere on the body surface. Nowadays, locations related to modern heat sources such as laptops and cellphones have been described [2]. Clinical suspicion is key, but histopathological evaluation may help rule out other disorders [3]. EAI can seldom lead to squamous cell carcinoma, Merkel carcinoma, and marginal zone B-cell lymphoma [4]. Differential diagnoses include livedo reticularis and racemosa (and all the diagnostic possibilities thereof), poikiloderma and lymphoma. Removal of the heat source is the mainstay of treatment. Dyschromia might improve with laser therapy, depigmentation therapies or topical retinoids, albeit usually permanent.
Conclusion
Medical history itself continues to be crucial in a myriad of dermatological conditions, such as EAI. Histopathology may aid in the differential diagnosis or to rule out complications in doubtful cases. Avoidance of the heat source and follow-up are recommended.
Declarations
Acknowledgments: none.
Funding sources: none.
Ethics statement: written informed consent was obtained from the patient.
Conflict of interest: authors declare no conflict of interests for this article.
References
- Chandra A, Sil A, Das S, Chakraborty U. Erythema ab igne: A cutaneous marker of prolonged thermal exposure. BMJ Case Rep. 2023; 16(8): e256612.
- Brazzelli V, Grassi S, Barruscotti S, Croci G, Borroni G. Erythema ab igne induced by laptop computer: An emerging disease among adolescents? G Ital Dermatol Venereol. 2020; 155(1). Available from: https://www.minervamedica.it/index2.php?show=R23Y2020N01A0099
- Segurado Tostón N, Puebla Tornero L, Revilla Nebreda D, Santos-Briz Terrón A. Eritema ab igne: correlación clínico-patológica en una serie de 5 pacientes y revisión de la literatura. Actas Dermo-Sifiliográficas. 2023; 114(4): 356-9.
- Wipf AJ, Brown MR. Malignant transformation of erythema ab igne. JAAD Case Rep. 2022; 26: 85-7.