
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Laparoscopic-assisted vaginoplasty in complex congenital urogenital anomaly: A case report
Chenglu Qin*; Pohching Lee; Jinqiu Shi
Department of Obstetric and Gynaecology, Luohu Hospital, Shenzhen 518001, China.
*Corresponding Author : Chenglu Qin
Department of Obstetric and Gynaecology, Luohu Hospital, Shenzhen 518001, China.
Tel: +8613622355101;
Email: clqin@163.com
Received : May 10, 2024
Accepted : May 28, 2024
Published : Jun 04, 2024
Archived : www.jcimcr.org
Copyright : © Chenglu Q (2024).
Abstract
We present a case report of a 15-year-old girl diagnosed with congenital vaginal atresia with ureteral bud and urethral anomaly. This case describes surgical selection and its long-term management. We used a laparoscopic-assisted vaginoplasty technique, which involved water infusion to separate the rectovesical plane and using the pedicle flap from the hematocolpos to cover the neovagina walls in high distal vaginal atresia. This technique has been adopted since 2015 and reported one successful pregnancy with a full-term live birth last year. Additional procedures in this case include the reconstruction of urethral and stent localization on both abnormal ureters. A detailed surgical description of our technique was elaborated, and the successful surgical approach was highlighted, even in the complexity of urogenital anomaly in this case.
Citation: Chenglu Q, Pohching L, Jinqiu S. Laparoscopic-assisted vaginoplasty in complex congenital urogenital anomaly: A case report. J Clin Images Med Case Rep. 2024; 5(6): 3093.
Introduction
Female reproductive tract develops in close association with many other organ systems. Understanding the embryology and anatomy of Müllerian structures is essential to ensure a complete workup [1]. The Müllerian structures derive from the primitive mesoderm, give rise to the fallopian tubes, uterus, cervix, and upper two-thirds of the vagina as to the heart, lungs, and urogenital system. The Müllerian ducts develop near the mesonephric ducts that eventually form the urinary tract and trigone of the bladder. The external genitalia and lower third of the vagina develop from the urogenital sinus, derived from primordial ectoderm. The ureters, which have formed as outgrowths of the mesonephric ducts, enter the bladder at the base of the trigone. As the bladder develops from the urogenital sinus, it absorbs the caudal parts of the mesonephric ducts, becoming the trigone of the bladder. Embryology variation in between ureteric bud and the urogenital sinus insertion could cause inadequate submucosal tunnel length of the intramural ureter in creating a mechanical antireflux mechanism [2]. Failure to fuse with the sinovaginal bulb or canalization of the MülMüllerian ducts or vaginal plate, vaginal atresia can occur. This case described surgical treatment of congenital vaginal atresia with ureteral bud anomaly and urethral malformation.
Case report
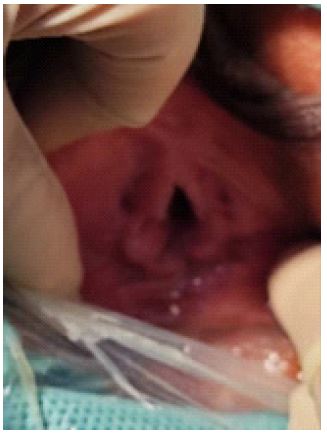
A 15-year-old girl presented with primary amenorrhea and six days of cyclical lower abdomen pain. From further history, the child has had intermittent urinary stress incontinence since ten years ago but did not seek medical advice till recently. Her developmental milestone was normal with no related family history. Secondary sexual characteristic started since three years ago, thelarche and pubarche stage III. Examination noted 12 weeks size uterus with no other palpable mass. Perineum examination revealed normal female features of the clitoris, labia majora, and minora, except enlarged urethral opening and no vaginal opening seen (Figure 1). Distance between the urethral opening to the posterior fourchette was about 1.5 cm. On rectal examination, the mass was felt compressing from the anterior wall 3 cm away from the vaginal vestibule. Pelvic ultrasound and Magnetic resonance imaging revealed a normal-shaped uterus of 6.1 x 4.7 x 3.8 cm, endometrial thickness of about 18 mm, cervical canal dilatation of about 13 mm diameter, and hematocolpos measuring 6.7 x 6.5 x 6.0 cm; distance between hematocolpos to the vestibule measuring 3.85 cm (Figure 2). Renal ultrasound and Computerized tomography urogram reported bilateral dilated ureters with abnormal ureterovesical insertion near the proximal urethral and bilateral hydronephrosis. Bilateral ureters measuring 8 to 15 mm with vesicourethral reflux Grade IV in International Reflux Grading system [2]. Renal profile and hormonal profile were within normal range for age. Preoperative counseling was performed with the urology team, and laparoscopic uterovaginoplasty, hysteroscopy, and cystoscopy with bilateral ureter stent insertion proceeded. Ureteral reimplantation was to be arranged at a later time.
Surgical procedure
The patient was instructed to follow a liquid-only diet for 1-2 days and a bowel cleanse one day before the surgery. A prophylactic antibiotic was given 30 minutes prior to the procedure. The urology team performed the pigtail insertion on both dilated ureters. During cystoscopy, a short urethra of about 2 cm and a normal bladder surface were identified, but the cavity was being compressed by the hematocolpos. Both ureter openings were noted as dilated until the kidney calyces and were located near the proximal urethral junction. A urinary catheter was inserted. Pneumoperitoneum was created up to 11 mmHg. A 10 mm primary port was placed as a camera port at the umbilical, while three 5 mm secondary ports were placed in the right iliac fossa, left lumbar, and left iliac fossa for operational purposes. The findings showed minimal adhesion between the adnexal and pelvic walls, with a 14 weeks size uterus. The vesicouterine layer was separated until visualization of the hematocolpos.
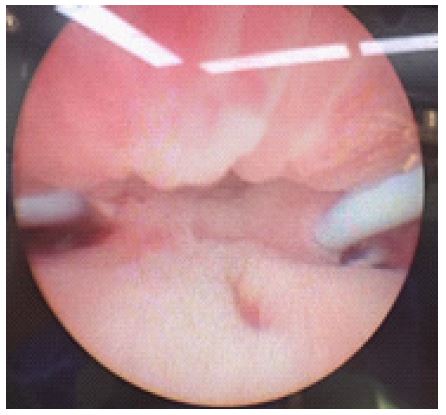
From the vagina approach, urethra reconstruction was performed post-pigtail insertion of both ureters (Figure 3). Utilizing water separation, the urethra was further separated from the blind-end vaginal vestibule, and sharp dissection was performed over the vaginal posterior to the urethra. It was then interrupted sutured with absorbable suture 3/0 to lengthen the urethra further.
Saline infusion was carried out using a veress needle, directed in between the vesicourethral and hematocolpos planes. To minimize rectal injury while inserting the needle, a finger was introduced into the rectum and touched the lower edge of the hematometra that compressed anteriorly to the rectum space to provide guidance. With direct laparoscopic visualization, the needle tip should be seen above the hematocolpos and bladder. Blood stains on the urine catheter were checked for early detection of urethra or bladder injury. Once the needle reached the site, saline was infused to expand the space until it became translucent, and the veress needle gradually penetrated it.
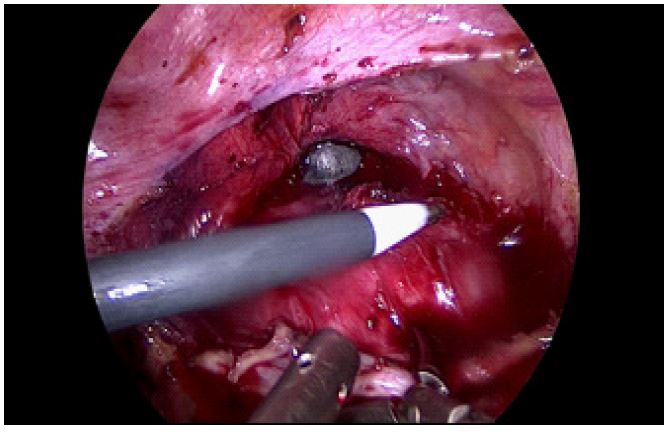
A laparoscopic suction was inserted through the secondary port and met the veress needle from the vagina. The suction acted as a guide, following the track created by the veress needle as it was removed from the vagina. An artery forceps was placed at the tip of the laparoscopic suction that was visible from the introitus. The suction was withdrawn while the tip of the artery forceps followed through the created space, expanding it further. The space was subsequently enlarged with Luohu dilators from size 1 to size 6 (22 mm till 35 mm diameter) to fit a vaginal passage of at least two finger breaths (Figure 4).
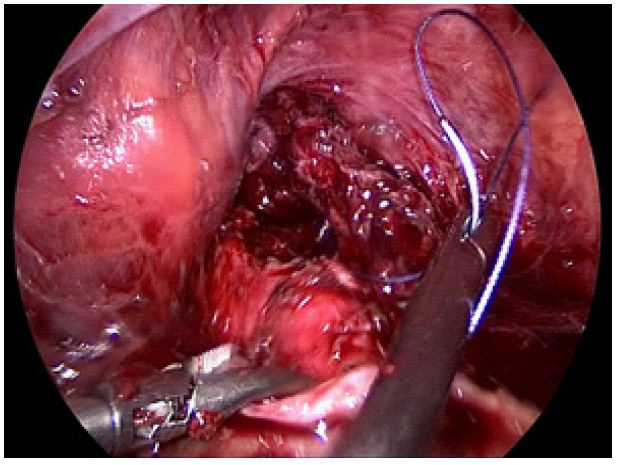
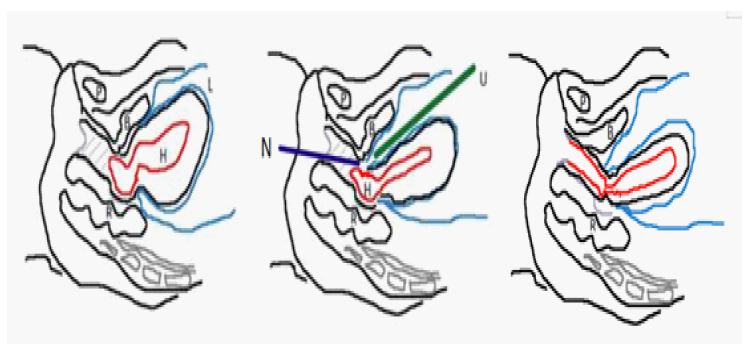
The uterine incision proceeded after the creation of the neovagina space since blood-free visualization was required to avoid unintended tissue injury. A 4 cm horizontal incision was made over the hematocolpos to create a posterior and anterior flap (Figure 5). The anterior flap was secured with absorbable suture 1/0, and the suture was brought to the vagina, and the same procedure was performed on the posterior flap. Both hematocolpos flaps were then pulled down to be sutured to the introitus. Diagram of the surgical procedure described (Figure 6).
Outcome
The endometriotic lesion at the uterine wall and peritoneal without involvement of adnexal showed the early stage of endometriosis with lesser detrimental impact on her future fertility. The operative time was 70 minutes, and the operative blood loss was 100 mL. A lengthy piece of gauze was inserted into the vagina and was to be kept for five days. A prophylactic antibiotic was given for a week. No postoperative infections or blood transfusions were documented. The urine catheter was kept for ten days with subsequent co-management with the urology team. Inpatient vaginal dilatation was performed under close supervision until discharge and warranted regular review.

Discussion
Based on the American Fertility Society Classification of Mullerian Anomalies, vaginal anomaly falls under partial or complete vaginal agenesis [3]. The VCUAM classification technique has a more comprehensive and detailed representation of vaginal abnormality, which includes septate, stenosis of the introitus, hypoplasia, atresia with or without sinus urogenitalis [4]. According to Ruggeri et al. 167 females with vaginal malformations have been observed, suggesting six types of vaginal atresia, including cloaca anomaly [5]. In our center, vaginal atresia was classified as distal vaginal agenesis or high distal vaginal agenesis with or without associated concomitant anomaly. High distal vaginal agenesis occurs if the atretic segment is longer than 3 cm [6] or if the atresia extends beyond the introitus by more than 3 cm, while distal vaginal atresia is less than 3 cm.
In distal vaginal agenesis, the vaginal approach was feasible. Needle-guided aspiration proceeded at the traces of the hymen and towards the lower edge of the hematocolpos while a finger stayed at the rectum to guide the direction. The incision of the hematocolpos was expanded, and the edge of the wall was pulled down to be sutured with the introitus. Regular vaginal dilation or a mold was required in both types of vaginal agenesis to maintain patency.
The operative challenges and recurrence are greatly exacerbated in high distal vaginal atresia. High distal vaginal atresia, in this case, was unable to be addressed with this technique due to the long atretic segment. Failure in treatment, as well as the risk of bleeding and organ injuries, were high. In this case, we adopted the laparoscopic technique of using a veress needle to act as a guide in creating neovagina space and hematocolpos flap covering the neovagina. This method has been used in our center in high distal vaginal atresia with promising results in mitigating surgical-related risks. Experience-based, the hematocolpos wall is equipped with strong elasticity and plasticity that allows grafting. It possessed an alternative physiological alternative covering the congenital defect and conforming a neovagina in a restricted space. The size of the hematocolpos varies depending on the vaginal atresia variation and the individual building of the cyclical menstruation quantity. Preoperative imaging assisted in the prediction. The more considerable hematocolpos expansion will ease its identification and adequacy in covering the neovagina of the pedicle flap.
Surgical expertise is required to perform precise dissection between the uterus and the bladder. The use of laparoscopy helps in achieving precise separation and hemostasis in a small space. Water pressure infusion is used with the veress needle from the vaginal and direct laparoscopic visualization to locate and separate the rectovesical space. Once the neovaginal channel is created by the veress needle, the space is gradually dilated with vaginal dilators to create more even expansion instead of using digital dissection. Blood-free visualization can be achieved if the neovagina is created before the hematocolpos incision. Our laparoscopic abdominovaginal approach involves less tissue handling than the vaginal approach alone.
The timing of surgery was determined based on the patient’s and family’s preferences, as well as their long-term postoperative commitments. Failure to regularly dilate the vagina after surgery can lead to a high risk of vaginal stenosis. Postoperative care could also be challenging for a young patient. To prevent restenosis until sexual activity begins, regular vaginal dilation was required. Alternatively, menstrual suppression and delaying surgery until the patient reaches maturity in decision-making and postoperative care could be considered. Our center’s experience suggests that the hematocolpos flap could provide a smooth physiological surface for the neovagina wall, reducing pain during dilation as well as mitigating the risk of restenosis. Even with the added complexity of a post-urethral intervention, which required extra care, vaginal dilation was still feasible in this case. Inpatient vaginal dilation was supervised for one to two weeks after surgery, and satisfactory self-dilatation was achievable.
One limitation of this method is that it was conducted at a single center and follow-up is required to assess its outcome. Last year, a successful pregnancy with a full-term cesarean birth was reported since adopting this technique for high distal vaginal atresia. This surgical procedure is suitable for vaginal atresia with the availability of the expanded hematocolpos cyst wall to be utilized as a pedicle flap. Inherent limitation to this technique is the possibility of insufficient hematocolpos flap to be pulled down, as in complete vaginal atresia. In such cases, alternative measures such as the use of tissue-engineered biomaterial, peritoneum, biological graft, and split skin graft or a two-step procedure with prior vaginal dilation could be employed, depending on the anatomy and concomitant anomalies [7,9]. Studies were reported on the grafts with adherence to postoperative dilation in vaginoplasty [10,11].
Not only pertaining to this complex case, attention for post-repair healing as well as long-term monitoring of the patient’s medical, psychosocial condition, and sexual function is required.
Conclusion
Comprehensive evaluation, including examination, preoperative imaging, and preoperative counseling, is crucial in selecting surgical procedures. In this case, we have described our surgical technique and method to prevent excessive tissue handling and surgical complications.
Declarations
Funding: This work was supported by the National Congenital Müllerian Anomaly Research Program of Luohu People’s Hospital-affiliated University for publication fees only. Serial No: 2021YFC2701401.
Patient consent: The review was approved by the Institutional Review Board of Shenzhen Luohu Hospital. Written informed consent was provided by the patient and family at consultation and all agreed that data and images could be included in the study and publication.
Author contribution statement: CL analyzed the results, performed the surgical procedures, reviewed the manuscript, and supervised the work. PC designed the overall study, analyzed the data, reviewed the literature and wrote the manuscript. JQ performed the surgical procedures and reviewed the manuscript.
Conflict of interest: The authors declare that no conflicts of interest associated with this publication.
References
- Acién P, Acién M. The history of female genital tract malformation classifications and proposal of an updated system. Hum Reprod Update. 2011; 17(5): 693-705.
- Duckett JW, Bellinger MF. A plea for standardized grading of vesicoureteral reflux. Eur Urol. 1982; 8(2): 74-7.
- Samantha M. Pfeifer, M.D., Marjan Attaran, M.D., et al. ASRM mullerian anomalies classification 2021
- Oppelt P, Renner SP, Brucker S, et al. The VCUAM (Vagina Cervix Uterus Adnex Associated Malformation) classifi cation: a new classifi cation for genital malformations. Fertil Steril. 2005; 84: 1493-7.
- Ruggeri G, Gargano T, Antonellini C, Carlini V, Randi B, Destro F, et al. Vaginal malformations: a proposed classification based on embryological, anatomical and clinical criteria and their surgical management (an analysis of 167 cases). Pediatr Surg Int. 2012; 28: 797-803
- Mansouri R,Dietrich JE. Postoperative course and complications after pull-through vaginoplasty for distal vaginal atresia. J Pediatr Adolesc Gynecol. 2015; 28(6): 433-436.
- Kashimura T, Takahashi S, Nakazawa H. Successful management of a thick transverse vaginal septum with a vesicovaginal fistula by vaginal expansion and surgery. Int Urogynecol J. 2012; 23: 797-9.
- Shen F, Zhang XY, Yin CY, Ding JX, Hua KQ. Comparison of small intestinal submucosa graft with split-thickness skin graft for cervicovaginal reconstruction of congenital vaginal and cervical aplasia. Hum Reprod. 2016; 31(11): 2499-2505.
- Qin C, Luo G, Du M, Liao S, Wang C, Xu K, Tang J, Li B, Zhang J, Pan H, Ball TW, Fang Y. The clinical application of laparoscope-assisted peritoneal vaginoplasty for the treatment of congenital absence of vagina. Int J Gynaecol Obstet. 2016; 133(3): 320-4. Epub 2016 Mar 2. PMID: 27087418.
- Zhang Y, Chen Y, Hua K. Outcomes in patients undergoing robotic reconstructive uterovaginal anastomosis of congenital cervical and vaginal atresia. Int J Med Robot. 2017;13(3): 1821.
- Zhang X, Qiu J, Ding J, Hua K. Comparison of neovaginoplasty using acellular porcine small intestinal submucosa graft or Interceed in patients with Mayer–Rokitansky–Küster–Hauser syndrome. Arch Gynecol Obstet. 2019; 300(6): 1633-6.