
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Glaucoma screening in patients with megalopapilla
Michael Gaspari1*; Muhamad Festok1; Jannah Chaudhry2
1Trinity Health Mid-Atlantic, Nazareth Hospital, Department of Ophthalmology, Philadelphia, PA, USA.
2IC Laser Eye Care, Bensalem, PA, USA.
*Corresponding Author : Michael Gaspari
Trinity Health Mid-Atlantic, Nazareth Hospital, Department of Ophthalmology, Philadelphia, PA, USA.
Email: michaelgaspari@gmail.com
Received : May 09, 2024
Accepted : May 29, 2024
Published : Jun 05, 2024
Archived : www.jcimcr.org
Copyright : © Gaspari M (2024).
Abstract
This report discusses the diagnostic challenges and management considerations in a 69 year old female presenting with Megalopapilla (MP) and potential glaucoma. MP is rare and benign condition marked by an enlarged optic nerve head with an anomalous disc shape. The differential diagnosis includes glaucoma and glaucoma like pathologies along with optic nerve coloboma, staphyloma and morning glory syndrome. Clinical examination in our case revealed an enlarged and pallorous optic nerve head, with a cup-to-disc ratio of 0.9 suggestive of glaucoma. A thick Retinal Nerve Fiber Layer (RNFL) was observed on optic nerve Optical Coherence Tomography (OCT) which is a common finding in megalopapilla. An enlarged blind spot was also noted on Humphrey Visual Field (HVF) testing. Despite the benign nature of megalopapilla, a comprehensive glaucomatous work-up is warranted due to associated structural abnormalities and potential vision-threatening complications. This work-up should include a baseline ocular exam along with ON-OCT and HVF examinations. Understanding the clinical characteristics and diagnostic modalities for megalopapilla is crucial for accurate diagnosis and appropriate management to prevent vision loss.
Citation: Gaspari M, Festok M, Chaudhry J. Glaucoma screening in patients with megalopapilla. J Clin Images Med Case Rep. 2024; 5(6): 3097.
Short report
The patient is a 69-year-old female with past ocular history significant for Hypertensive retinopathy OU, past ocular surgical history of bilateral 8 mm lateral rectus resection (2012), cataract extraction with PCIOL placement OU (2014), Upper and Lower Eyelid Blepharoplasty (2015). YAG posterior capsulotomy OU (2016), and, past medical history significant for hypertension, asthma, and osteoarthritis, colon cancer s/p colon resection (2018), (no longer on chemotherapy), family history negative for glaucoma or other significant ocular pathologies, who presented to the office for foreign body sensation. Ocular examination revealed visual acuity in both eyes (without correction) of 20/30. Pupil examination demonstrated a 2+ APD OS but otherwise within normal limits. External ocular motility was full, with an alternating exotropia OS, no visual field defect was found by confrontational field. Color testing demonstrated 8/8 OD and 7/8 OS. Intraocular pressure was measured at 12 OD and 13 OS. Slit-lamp examination demonstrated an unremarkable adenexa, with well healed surgical scars noted on the upper eyelids near the crease, and subciliary. Corneal examination showed inferior SPK greater on the left than right. Upon examination of the conjunctiva, conjunctival chalasis was noted, and a large 2 x 2 mm dellen was found near the limbus of both the right eye. The anterior chamber was deep and quiet, with slight sectoral Iris atrophy noted in the right eye, extending from the 6:00 position to the 9:00 position and on the left eye at the 3:00 position. Posterior chambers both contained a three piece IOL with an adequate nd: YAG posterior capsulotomy.
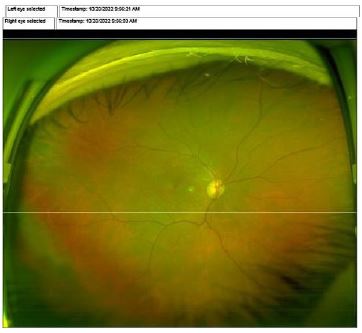
Dilated examination of the posterior pole of both eyes showed a clear vitreous with degeneration. The optic nerve of the right eye was normal in size with a 0.6 cup-to-disc size. The optic nerve of the left eye was noted to be roughly twice the size of the fellow nerve, with an abnormal shape and slightly pallorous color. The cup-to-disc size was 0.9-0.95 with a superiorly displaced cup, and optic nerve margins appearing nearly completely obliterated (Type 2 variant). The vessels of both eyes were noted to be attenuated, with normal appearing peripheral fundi and macula.
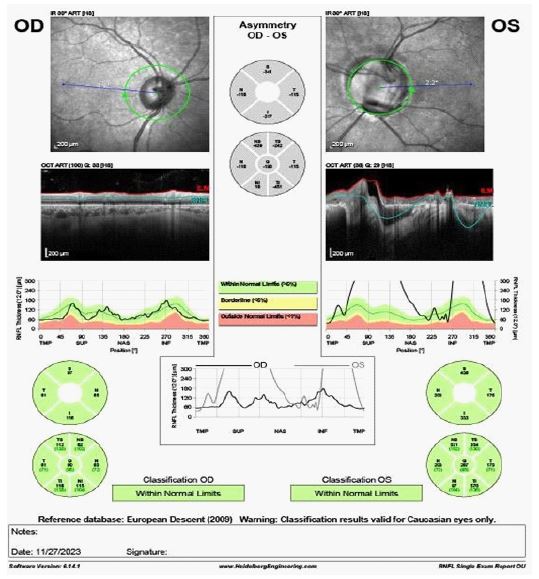
Humphrey Visual Field were grossly normal OD, but showed a slightly enlarged blind spot OS. ON OCT did not demonstrate any thinning OU, but did highlight severe segmental thickening of the RNFL OS and a superiorly displaced cup. These tests were repeated and results were unchanged.
Megalopapilla (MP) is a rare benign condition that is defined mainly by an enlarged optic nerve head and abnormal appearing disc shape The differential diagnosis should include glaucoma, Optic nerve coloboma staphyloma, and morning glory syndrome. It is described as an enlarged disk with a surface area >2.50 mm, with any associated structural abnormalities. ON OCT usually demonstrates enlarged disc area, rim area, cup size and cup to disc ratio [1,2] ON OCT also usually demonstrates normal RNFL thickness of the megalpapilla nerve in comparison to normal nerve RNFL [3]. While megalopapilla does not usually cause vision loss, the high C/D ratio, thin neuroretinal rim and disc pallor should always warrant a full glaucomatous work-up, due to their clinically similar appearances. This work-up should include both Optical Coherence Tomography (OCT) and Humphrey Visual Field (HVF.) examinations. OCT of the RNFL in eyes with megalopapilla often demonstrates a thicker than normal RNFL, and HVF can show an enlarged blind spot, both findings demonstrated our patient.

References
- Lee HS, Park SW, Heo H. Megalopapilla in children: A spectral domain optical coherence tomography analysis. Acta Ophthalmol. 2015; 93(4): e301-5. doi: 10.1111/aos.12545.
- Sampaolesi R, Sampaolesi JR. Large optic nerve heads: megalopapilla or megalodiscs. Int Ophthalmol. 2001; 23: 251-257.
- Da Costa AM, Cronemberger S. Optic disc and retinal nerve fiber layer thickness descriptive analysis in megalopapilla. J Glaucoma. 2014; 23: 368-371.