
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Management of Crohn’s disease and its complexities: A case report
*Corresponding Author : Niragh Sikdar
Department of Medicine, Medical College & Hospital Kolkata, Kolkata, India.
Email: niraghsikdar@gmail.com
Received : May 15, 2024
Accepted : May 30, 2024
Published : Jun 06, 2024
Archived : www.jcimcr.org
Copyright : © Sikdar N (2024).
Abstract
Crohn’s Disease (CD) and its complexities are explored through a case report and literature review, shedding light on the multifaceted nature of this chronic inflammatory gastrointestinal disorder. Characterized by unpredictable flare-ups and remissions, CD affects various segments of the gastrointestinal tract, leading to symptoms such as abdominal pain, diarrhea, and weight loss, significantly impacting patients’ quality of life. The intricate interplay of genetic, environmental, and immune factors contributes to the pathogenesis of CD, manifesting in diverse clinical phenotypes and requiring a nuanced therapeutic approach. This study emphasizes the challenges in managing CD, encompassing a range of treatments from medications to surgical interventions while underscoring the intricacies and potential complications encountered, particularly in the postoperative phase, to optimize patient care and outcomes in this complex inflammatory condition. This report delves into the complexities of Crohn’s disease through the case of a 20-year-old male. It illustrates the diverse symptoms, treatment modalities, and intricate challenges faced, notably post-surgical complications like small bowel leaks. Emphasizing the disease’s unpredictable nature and significant impact on patient’s lives, it underscores the necessity for vigilant postoperative care to improve outcomes in this intricate inflammatory disorder.
Keywords: Crohn’s Disease (CD); Ileocecectomy; NF-κβ pathway; Laparotomy; Intra-abdominal abscesses.
Citation: Sikdar N. Management of Crohn’s disease and its complexities: A case report. J Clin Images Med Case Rep. 2024; 5(6): 3100.
Introduction
The term ‘Inflammatory Bowel Disease’ is used to describe Crohn’s Disease (CD) and Ulcerative colitis which are immunologically mediated inflammatory diseases of the gastrointestinal tract. Crohn’s disease is often diagnosed at a young age and has a chronic course coupled with acute flare-ups. Any part of the gastrointestinal system can be impacted by Crohn’s disease with roughly one-third of patients being involvedlimited to the small bowel, particularly the terminal ileum; another 20% have involvement limited to the colon; and approximately 50% have involvement involving both the colon and small bowel. Most patients go through unpredictable remissions and relapses, and there is no known cure leading to a deficient quality of life [1]. IBD is usually characterized by dysregulation of the NF-κβ pathway and proteins that regulate it, which results in uncontrolled inflammation and impaired immunity. In both CD and UC, there is a rise in the levels of proinflammatory cytokines that are controlled by NF-κβ [2].
In IBD, particularly in CD, the gut microbiota is known to have an impact on how the inflammatory response is developed. Typically, the inflammation is transmural, and biopsies may reveal granulomas with a discontinuous distribution along the longitudinal axis during pathological evaluation. Intestinal fistulas, inflammatory tumors, and intra-abdominal abscesses are some of the irreparable tissue damages caused by this inflammatory process [3], Crohn’s disease flare-ups are commonly accompanied byfever, weight loss, anemia, diarrhea (which may include blood and mucus), flatulence/bloating, and right lower quadrant abdominal pain. Perianal abscess, perianal Crohn’s disease, and cutaneous fistulas are often detected in severe cases [4], mild to moderate CD is often treated with drugs such as mesalamine, immunomodulators, and steroids whereas severe CD requires additional biologic drugs such as infliximab and adalimumab [5]. Patients with CD have a wide range of surgical indications. Given that CD cannot be cured, there must be rigorous guidelines for surgical indications, and the procedure should be as limited and less invasive as feasible. Since restricted bowel resection and strictureplasty are safe and useful, the once-popular bypass procedure has been almost abandoned [6]. Surgery provides more definitive treatment for CD, but it comes with several complications, the most severe of which include wound infections at the surgical site, anastomotic leaks (both acute and chronic), and anastomotic strictures. Anastomotic sinus can result from a persistent anastomotic leak, while an abscess or sepsis can be caused by an acute leak. Reducing postoperative infection problems requires preoperative treatment that includes nutritional support, intravenous antibiotics, weaning off immunosuppressive drugs, and, if present, percutaneous drainage of abscesses [7].
We present the case of a 20-year-old male who was recently diagnosed with CD, presenting with worsening abdominal pain associated with nausea and bloating. Imaging tests revealed small bowel obstruction along with chronic strictures and the patient was prepared for laparoscopic ileocecectomy after surgical evaluation. Post-operation, the patient complained of abdominal pain along with fever, chills, and tachycardia for which exploratory laparotomy was carried out. An intra-abdominal small bowel leak as well as considerable intra-peritoneal contamination with small bowel feculent spillage was detected.
Case presentation
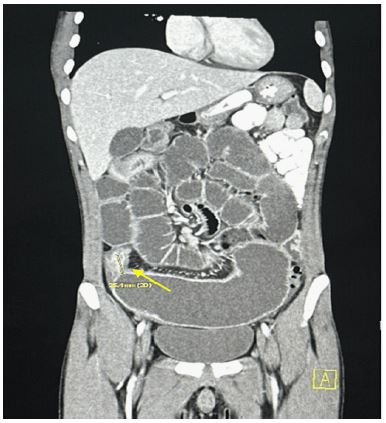
A 20-year-old male with a past medical history of Crohn’s disease presented with abdominal pain. The patient reports progressively worsening cramping diffuse 8/10 abdominal pain associated with nausea and bloating for the last 3 days before admission. The rest of his review of systems was unremarkable. His vital signs including temperature were within normal limits. Physical examination was notable for a mildly distended abdomen with minimal tenderness to deep palpation. His family history is significant for Crohn’s disease in his sister. He was recently diagnosed with Crohn’s disease after multiple visits to the emergency department for intermittent cramping abdominal pain with nausea and vomiting. At that time, Colonoscopy revealed ileitis with narrowing of the terminal ileum, and he was started on prednisone 35 mg daily and Stelara infusions. 2 months before his current admission, a Computed Tomography (CT) abdomen and pelvis with oral and intravenous contrast showed gradual dilation of the distal jejunum with markedly dilated loops of ileum measuring up to 5.7 cm as seen in Figure 1.
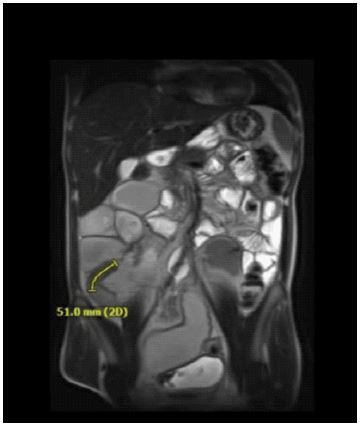
Magnetic Resonance Enterography (MRE) then also demonstrated actively inflamed and narrowed terminal ileum causing marked upstream dilation, as well as findings suggestive of active inflammation of the dilated small bowel as seen in Figure 2.
Initial blood workup was remarkable for hemoglobin of 9.8 without leukocytosis. CT abdomen and pelvis with contrast revealed a known transition point at the terminal ileum (consistent with the most recent MRE demonstrating chronic stricture) with worsening upstream dilatation measuring at 7.3 cm in diameter and small bowel obstruction. The patient was admitted to the surgery ward and planned for further surgical evaluation for possible ileal resection. Prior to surgical evaluation, he was resumed on IV prednisone 40 mg and a Peripherally Inserted Central Catheter (PICC) line was inserted for Total Parental Nutrition (TPN), which slightly improved his symptoms as he started tolerating pain with having bowel movement and flatus. The patient then underwent laparoscopic ileocecectomy with ileostomy formation rather than anastomosis given the patient’s poor nutrition from chronic obstruction as well as high-dose steroids. Gross examination of the excised specimen (27 cm of ileum and 4 cm of cecum in length) demonstrated extensive ulceration and cobblestone appearance, and the pathology report revealed ulcerative transmural ileitis, consistent with the active phase of reported Crohn’s disease.
After the procedure, the patient complained of abdominal pain that was controlled with Patient-Controlled Analgesia (PCA). Following that, the patient had an episode of persistent tachycardia and oxygen desaturation down to 88% while on 2 liters of continuous nasal cannula oxygen, and labs were significant for worsening leukocytosis close to 20,000. CT chest, abdomen, and pelvis with contrast was notable for a new circumferential wall thickening and mucosal hyper enhancement, which likely reflected active disease or possible superimposed infectious enteritis, for which zosyn and fluconazole were started, and interventional radiology was consulted regarding low ostomy output. Paracentesis was subsequently performed with about 1400 cc of purulent fluid removed. The patient then developed a spike in fever (38.8°C), chills, tachycardia of 140, and worsening leukocytosis up to 23,000. CT abdomen and pelvis with oral and IV contrast was therefore conducted which revealed abdominal extravasation concerning postoperative small bowel leak as seen in Figure 3, and the patient underwent prompt exploratory laparotomy for small bowel evaluation and ileostomy revision.
Exploratory laparotomy was significant for an active 1 cm area of staple line dehiscence creating intra-abdominal small bowel leak at the site of the prior ileal staple line, as well as considerable intraperitoneal contamination with small bowel feculent spillage but without focal collections or abscesses. A considerable quantity of creeping fat along the ileum was noticed and at this point, it was noted that a considerable portion of the terminal ileum was inflamed. The surgeon then proceeded with resection of the inflamed bowel (measuring 18.1 cm in length) and the creation of a new end ileostomy. Given intra-abdominal contamination, the surgeon gave recommendations to wait at least six months before reversing the patient’s ostomy. After surgery, the patient was given a blood transfusion for low hemoglobin levels and continued antibiotics with the addition of fluconazole for persistent leukocytosis. CT chest, abdomen, and pelvis with contrast showed moderate to large ascites with blood products, for which paracentesis was performed and micafungin was started for coverage of Candida Krusei growing in the abdominal fluid. The patient’s energy level and ambulation gradually improved with white blood count down trending. He was eventually deemed to be stable for discharge on outpatient intravenous antibiotics with strict follow-up instructions and teaching on ostomy changing and draining. A follow-up Magnetic Resonance Enterography (MRE) done 2 months following his discharge showed a significant decrease in intra-abdominal and intra-pelvic fluid collections as seen in Figure 4.
The patient responded well to the treatment given and scheduled for further outpatient follow-up.
Discussion
Crohn’s disease, a chronic inflammatory ailment of the gastrointestinal tract, affords an impressive challenge in its control. Epidemiologically, it demonstrates a worldwide distribution with a higher prevalence in Western counties, impacting people across a huge age spectrum [8]. The etiology entails a complex interaction of genetic, environmental, and immune factors, mainly to transmural inflammation affecting any part of the gastrointestinal tract [9]. Common signs and symptoms consist of abdominal pain, diarrhea, weight reduction, and fatigue, substantially compromising sufferers’ high-quality of life [8]. Despite sizeable development in comprehending its pathogenesis, therapeutic alternatives, and surgical interventions, Crohn’s ailment stays a multifaceted entity worrying a nuanced technique.
The literature on Crohn’s ailment is extensive, underscoring the multifaceted nature of the disease. The ailment’s heterogeneity is properly documented, providing with various clinical phenotypes, starting from inflammatory to structuring and penetrating forms [10]. The chronic and relapsing nature of Crohn’s disease necessitates a multifaceted therapeutic approach, encompassing immunosuppressive agents, corticosteroids, and biologics [11]. Surgical interventions, together with bowel resection, strictureplasty, and stomas advent, play a pivotal role in managing complications and enhancing the overall quality of life for affected individuals [12]. Despite therapeutic improvements, demanding situations persist in achieving sustained remission and preventing disease recurrence, prompting ongoing exploration into novel therapies, together with personalized remedy strategies and microbiome-based interventions [11,12].
The provided case contributes to the literature by means of offering a unique clinical perspective. The affected person’s records of Crohn’s ailment, complex via chronic inflammatory modifications inside the terminal ileum, aligns with present literature emphasizing the unpredictable and heterogeneous nature of the disease. However, the individuality of this case lies within the elaborate series of occasions following surgical intervention. The development of a small bowel leak at the staple line, intra-stomach contamination, and next complications adds a layer of complexity no longer significantly explored in existing literature. While previous research acknowledges the potential want for surgery in Crohn’s disorder, this example underscores the difficult interaction among chronic infection, postoperative complications, and the demanding situations in reaching a favorable outcome [10-12]. The nuanced details of this situation offer treasured insights into probable complications and emphasize the need for vigilant postoperative monitoring and timely intervention to optimize affected person consequences within the context of this difficult inflammatory disorder. Understanding such nuances is pivotal for refining healing strategies and improving standard patient care in the challenging landscape of Crohn’s sickness [8,9].
Conclusion
Crohn’s disease poses a multifaceted challenge, impacting individuals across diverse demographics due to its complex etiology involving genetic, environmental, and immune factors. The case study underscores the disease’s heterogeneous nature and the intricate interplay between chronic inflammation, surgical interventions, and postoperative complications, notably a small bowel leak. These events highlight the gaps in understanding the complexities following surgical procedures in Crohn’s disease. Vigilant postoperative monitoring and timely interventions are crucial to mitigate complications and optimize patient outcomes in this challenging inflammatory condition, emphasizing the imperative for nuanced strategies to enhance patient care and therapeutic approaches in Crohn’s disease management.
References
- Marazuela García P, López-Frías López-Jurado A, Vicente Bártulos A. Acute abdominal pain in patients with Crohn’s disease: What urgent imaging tests should be done?. Radiologia (Engl Ed). 2019; 61(4): 333-336. 10.1016/j.rx.2018.12.003.
- Zaidi D, Wine E. Regulation of Nuclear Factor Kappa-Light-Chain-Enhancer of Activated B Cells (NF-κβ) in Inflammatory Bowel Diseases. Front Pediatr. 2018; 6: 317. 10.3389/fped.2018.00317.
- Petagna L, Antonelli A, Ganini C, et al. Pathophysiology of Crohn’s disease inflammation and recurrence. Biol Direct. 2020; 15(1): 23. 10.1186/s13062-020-00280-5.
- Fumery M, Pariente B, Sarter H, et al. Long-term outcome of pediatric-onset Crohn’s disease: A population-based cohort study. Dig Liver Dis. 2019; 51(4): 496-502. 10.1016/j.dld.2018.11.033.
- Targan SR. Biology of inflammation in Crohn’s disease: mechanisms of action of anti-TNF-a therapy. Can J Gastroenterol. 2000; 14(Suppl C): 13C-16C. 10.1155/2000/409396.
- Strong SA. Surgical management of Crohn’s disease. In. Holzheimer RG Treatment, Mannick JASurgical and Evidence-Based and Munich, Problem-Oriented and Zuckschwerdt (ed). 2001.
- Li Y, Zhu W. Common Complications of Surgery for Crohn’s Disease and Ulcerative Colitis. Interventional Inflammatory Bowel Disease: Endoscopic Management and Treatment of Complications. 2018; 273-286. 10.1016/b978-0-12-811388-2.00024-5.
- Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012; 142(1): 46-54.e42. 10.1053/j.gastro.2011.10.001.
- Levine JS, Burakoff R. Extraintestinal manifestations of inflammatory bowel disease. Gastroenterol Hepatol (N Y). 2011; 7(4): 235-41.
- Torres J, Mehandru S, Colombel JF, et al. Crohn’s disease. Lancet. 2017; 389(10080): 1741-1755. 10.1016/S0140-6736(16)31711-1.
- Lichtenstein GR, Loftus EV Jr, Isaacs KL, et al. Correction: ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am J Gastroenterol. 2018; 113(7): 1101. 10.1038/s41395-018-0120-x.
- Frolkis AD, Vallerand IA, Shaheen AA, et al. Depression increases the risk of inflammatory bowel disease, which may be mitigated by the use of antidepressants in the treatment of depression. Gut. 2019; 68(9): 1606-1612. 10.1136/gutjnl-2018-317182.