
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Anatomical variations in hepatic artery system in a North Indian population: A cross-sectional study using multi-detector computed tomography
Hasan Atif; Sachin Khanduri; Zaara Khan*; Rohit; Avani Kanojia; Akshay Aggarwal; Nishat Ara; Shaikh Jahangir Abdul Rauf; Sachin A. Goswami; Surbhi
Department of Radio-diagnosis, Era Medical College and Hospital, Lucknow, Uttar Pradesh, India.
*Corresponding Author : Zaara Khan
Department of Radio-diagnosis, Era Medical College and Hospital, Lucknow, Uttar Pradesh, India.
Email: drzaarakhan@yahoo.com
Received : May 14, 2024
Accepted : May 30, 2024
Published : Jun 06, 2024
Archived : www.jcimcr.org
Copyright : © Khan Z (2024).
Abstract
Background: The hepatic artery system exhibits significant anatomical variability, which is crucial for surgical planning and interventions. Understanding these variations within specific populations can enhance the precision of radiological assessments and surgical procedures.
Aim: To study the anatomical variations in the hepatic artery system using Multi-Detector Computed Tomography (MDCT) in a North Indian population.
Objectives: To determine the variation in the branching pattern of the hepatic artery using MDCT.
To document the prevalence of different types of anatomical variations in the study population.
Methods: A cross-sectional study was conducted over a period of twenty-four months in the Department of Radiodiagnosis, in collaboration with the Departments of Surgery and Medicine at Era’s Lucknow Medical College & Hospital, Lucknow. Patients who met the inclusion criteria were clinically examined, and their age, sex, and clinical profiles were noted. The study focused on the origin, path, and branches of the Common Hepatic Artery (CHA), Right Hepatic Artery (RHA), Left Hepatic Artery (LHA), as well as associated arteries like the left and right gastric, accessory hepatic, and mesenteric arteries. Anatomical variations were classified according to established classifications, such as Michel’s classification.
Results: MDCT revealed normal (Type 1) anatomy in 80% of the cases. Anatomical variations were present in 20% (n=30) of the study population. The most common variant was Type 3 (n=7, 4.7%), followed by Type 9 (n=5, 3.3%), Types 2 and 6 (n=4, 2.7% each), Type 5 (n=3, 2%), and Types 4 and 7 (n=2, 1.3% each). One case (0.7%) exhibited Michel’s Type 8 anatomy, while two cases (1.3%) did not conform to any described types in Michel’s classification.
Conclusion: This study highlights the significant prevalence of anatomical variations in the hepatic artery system within a North Indian population. MDCT proves to be an effective tool for identifying these variations, which is essential for optimizing surgical and radiological practices.
Citation: Atif H, Khanduri S, Khan Z, Rohit, Kanojia A, et al. Anatomical variations in hepatic artery system in a North Indian population: A cross-sectional study using multi-detector computed tomography. J Clin Images Med Case Rep. 2024; 5(6): 3101.
Introduction
Knowledge of hepatobiliary-vascular anatomy and its different variants is essential for surgical decision-making owing to its possible impact on peri-operative complications and overall surgical outcomes. The hepatobiliary-vascular anatomy comprises four components biliary tract or biliary tree is a system of narrow tubular structures connecting the liver, gall bladder, pancreas, and other associated structures and is responsible for production, storage, secretion, and transport of bile; arterial supply to the biliary tract; portal vein system and Hepatic venous system respectively. Several classifications are prevalent to describe anatomical variations. Variations in hepatic vascular anatomy are quite frequent. They are often said to be more of a rule than an exception. The incidence of variation in the portal vein is reported to be approximately 20.1%, that in the biliary duct is reported to be approximately 10.9% [1-3], and that in the hepatic artery is reported to be approximately 44% [4,5]. Knowledge regarding different variants of bilio-vascular anatomy holds a high clinical significance and awareness regarding their patterns in a specific population might be helpful in the prevention and management of biliary injuries during various surgical procedures [6]. Concerning gastro-hepato-pancreato-biliary pathologies, they might be useful in the appropriate utilization of surgical intervention while at the same time enhancing the favorable outcome and improving the patient experience. The normal branching pattern of the CT and the three main branches are the Left Gastric Artery (LGA), Common Hepatic Artery (CHA), and Splenic Artery (SA). The celiac axis and its branches supply the derivatives of the foregut, i.e. stomach, spleen, pancreas, liver, and part of the duodenum. The most common classical type of branching of CT is known as trifurcation and was first described by Haller in 1756 as tripus Halleri. The incidence of different celiac and hepatic artery anomalies was calculated depending on Uflacker’s and Michel’s classifications [7]. Gastrointestinal, hepatobiliary, and pancreatic cancers comprise nearly 26% of the total cancer burden and are responsible for 35% of cancer-related deaths globally [8]. Surgical resection is one of the most common methods for the management of these cancers [9]. Nearly half the cases of some common types of these cancers like hepatocellular carcinoma that comprise 90% of total primary liver cancer cases are diagnosed at early stages during surveillance and are curable through surgical intervention [10]. Similarly, nearly one-fifth to one-third of pancreatic cancer patients are candidates for surgery with very low perioperative mortality [11,12]. In gastric cancer cases, too, complete surgical resection with a standardized lymphadenectomy is the preferred curative measure [13] Despite promising results, surgery is often seen as an underutilized treatment modality in cases of gastro-hepato-pancreato-biliary malignancy [14,15]. In recent years, Multidetector Computed Tomography Angiography (MDCT Angiography) has emerged as a useful imaging modality for the evaluation of hepatic artery variations. It is highly accurate and reliable in the evaluation of the hepatic artery configuration [16].
Materials & methods
A cross-sectional study was carried out at the Department of Radiodiagnosis in collaboration with the Departments of Surgery and Medicine, Era’s Lucknow Medical College & Hospital, Lucknow for a duration of twenty-four months. Era’s Lucknow Medical College & Hospital is a tertiary care center with state-of-the-art infrastructure catering primarily to the socio-economically underprivileged suburban and rural population of Lucknow where patients scheduled for diagnostic procedures for various medical/surgical indications referred from Departments of Medicine and Surgery comprised of the study population. Clearance for carrying out the study was obtained from the Institutional Ethical Committee Era’s Medical College (Approval number: ELMC & H /RCELL, EC/2021/132), and informed consent was obtained from all the patients. The sampling frame of the study was bound by the following inclusion and exclusion criteria:
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Adults aged >18 were referred for abdominal CT by the Department ofMedicine and Surgery. | Previous hepaticor major abdominal surgery |
| Impairedrenal function | |
| Allergyto contrast media | |
| Pregnancy | |
| Hepaticmasses |
The sample size was calculated at the Department of Social & Preventive Medicine, Era’s Lucknow Medical College & Hospital, Lucknow. The sample size was calculated based on the proportion of cases with abnormal anatomy using the formula:
n = z2pq/L2
Where p = 26.2% the proportion of cases with abnormal anatomy [25].
q = 100 - p,
Type I error α=5 %, for the significance level of 95%.
Methodology
All the patients falling in the sampling frame and fulfilling the eligibility criteria were clinically examined and age, sex, and clinical profile were noted. Abdominal Computed tomography was performed using a 384-slice multidetector CT scanner (Somatom Force, Seimens Healthcare). Before IV contrast injection a Region of Interest (ROI) was kept over the abdominal aorta. Then Bolus of 15 ml per kg of iso-osmolar non-ionic iodinated contrast (Iohexol of 350 mg/ml) was injected into the antecubital vein at the rate of 5 ml/sec using a pressure injector followed by induction of 40 ml of saline chaser at the rate of 5 ml/sec. Images were post-processed on a workstation using Syngovia software that allowed the analysis of images. The examination was evaluated by radiologists. The origin, path, and branches of the Common Hepatic Artery (CHA), Right Hepatic Artery (RHA), Left Hepatic Artery (LHA), left and right gastric, accessory hepatic and mesenteric arteries were noted and classified according to Michel’s Classification [5].
Data analysis
Data so collected were analyzed using IBM SPSS 21.0 software. Data has been shown as numbers and percentages or mean + SD. The chi-square test was used to compare categorical/discrete data. Continuous data were evaluated using independent samples ‘t-test and ANOVA. A ‘p-value less than 0.05 indicated a statistically significant association.
Results
The present study was carried out to study the normal anatomy and variations in the hepatic arterial system using a multidetector CT scanner in a north Indian population. For this purpose, a total of 150 subjects falling in the sampling frame were enrolled. Out of which 87 were male and 63 were female. In the present study, a multidetector CT scanner revealed normal (Type 1) anatomy in most (80%) cases. Anatomical variations were seen in 30(20%) of the study population. Type 3 (n=7; 4.7%) was the most common anatomical variant followed by Type 9(n=5; 3.3%), Types 2 and 6(n=4; 2.7% each), Type 3 (n=3; 2%) and Type 4 and 7 (n=2; 1.3%) each. One (0.7%) case was with Michel’s type 8 anatomy. A total of two (1.3%) cases remained unclassified as they did not match any of the types described in Michel’s classification. Table 1 shows the case distribution of hepatic artery variations in our cases.
Table 1: Case distribution of hepatic artery variations in our cases.
| Type | No. of cases | Percentage |
|---|---|---|
| Type 1 | 120 | 80.0 |
| Type 2 | 4 | 2.7 |
| Type 3 | 7 | 4.7 |
| Type 4 | 3 | 2.0 |
| Type 5 | 2 | 1.3 |
| Type 6 | 4 | 2.7 |
| Type 7 | 2 | 1.3 |
| Type 8 | 1 | .7 |
| Type 9 | 5 | 3.3 |
| Unclassified | 2 | 1.3 |
The proportion of those with normal anatomy (Type 1) was higher in females (85.7%) as compared to that in males (75.9%), however, this difference was not significant statistically (p=0.137)
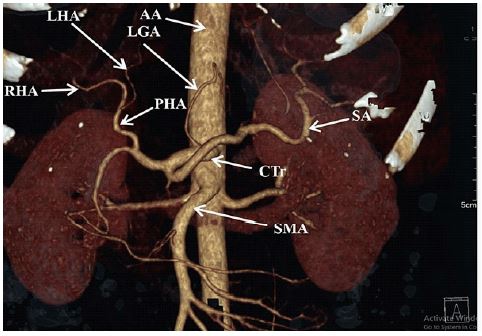
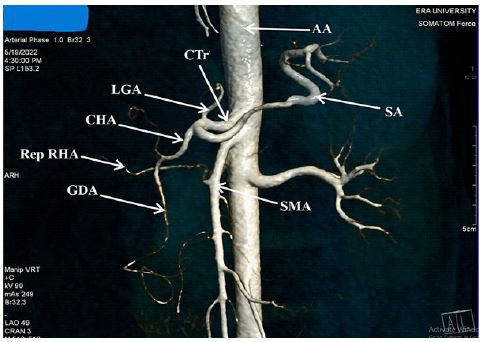
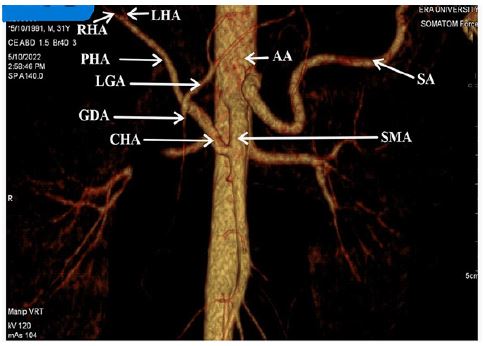
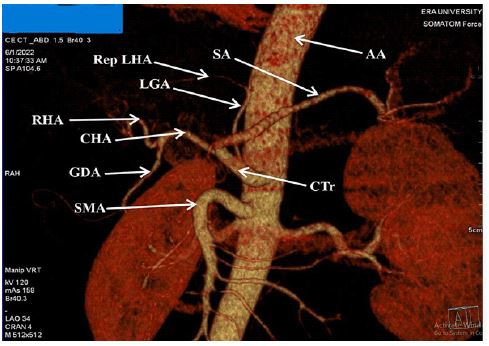
Figures 2-5 are showing the most common hepatic variants observed in our study.
Discussion
Hepatobiliary surgeries present unique challenges to the surgeons for the associated difficulties because of several anatomical variations in structures like bile and hepatic ducts and hepato-pancreato-biliary vasculature leading to which risk of intraoperative injury [17]. Several such surgeries are performed laparoscopically. The anatomical variations in the hepatic artery might be dependent on the patient’s genetic and environmental differences. With imaging techniques like sonography, computed tomography, and magnetic resonance imaging, non-invasive assessment has become feasible and has contributed tremendously. For this purpose, a cross-sectional study was carried out in which a total of 150 North Indian individuals (aged 18 to 80 years) were enrolled. A cross-sectional study is a type of observational study, it allows the investigator to investigate the prevalence of a disease or condition in a select sample randomly drawn from a population and to study the exposure and outcome at the same time [18]. In the present study, the age of the study population ranged from 18 to 80 years, and the mean age of patients was 43.90±17.01 years. There was the dominance of those aged >40 years (54.7%). The majority of patients were males (58%). The sex- ratio (M:F) of the study population was 1.38. In one study Choi et al [19] reported mean age as 60 years. A number of other studies just described the age range and did not report the mean or median age [20-22]. As such it is believed that age does not affect the hepatic arterial anatomy and hence, these workers did not consider it to be relevant to report it. As far as sex profile is concerned, most of the studies similar to the present study showed male dominance. However, there are few studies that have shown female dominance too [23,24]. In the present study, anatomical variations were seen in 30(20%) of the study population. Type 3 (n=7; 4.7%) was the most common anatomical variant followed by Type 9 (n=5; 3.3%), Types 2 and 6 (n=4; 2.7% each), Type 3 (n=3; 2%) and Type 4 and 7 (n=2; 1.3%) each. One (0.7%) case was with Michel’s type 8 anatomy. A total of two (1.3%) cases remained unclassified as they did not match any of the types described in Michel’s classification. The findings of the present study show a relatively lower prevalence of anatomical variations and a slightly different profile of anatomical variants, requisitioning the need to validate the results of the present study on a larger representative sample. In the present study, we found the prevalence of anatomical variations to be higher in males (24.1%) as compared to that in females (15.3%). In the present study, the risk of hepatic artery injury owing to aberrant anatomy could thus be reduced by 20%. Despite having an a priori sample size calculation approach, we feel that a larger sample size might have been more helpful, especially concerning the study of different types of anatomical variants and to justify some of the away-from-stream trends in the present study. The present study showed that a large proportion of the population has hepatic artery anatomical variations. Knowledge of these variations could help in better surgical and interventional planning.
The present study revealed normal (Type 1) anatomy in most (80%) cases. Anatomical variations were seen in 30(20%) cases. The mean age of patients having normal (Type 1) anatomy was 44.53±16.83 years whereas the mean age of patients showing anatomical variations was 41.37±17.77 years. However, there was no significant association between anatomical variations and age. The findings of the present study showed a high prevalence of normal hepatic artery anatomy in the North Indian population as revealed by MDCT. The findings of the study have high clinical relevance. The anatomical variations were unaffected by age and sex, hence showing the value and necessity of imaging modalities like MDCT in exploring the anatomical variations of the hepatic artery before planning any intervention.
References
- Atri M, Bret PM, Fraser-Hill MA: Intrahepatic portal venous variations: prevalence with the US. Radiology. 1992; 184: 157-158. 10.1148/radiology.184.1.1609075
- Cheng YF, Huang TL, Chen CL, Chen YS, Lee TY. Variants of the intrahepatic bile ducts: application in living-related liver transplantation and splitting liver transplantation. Clin Transplant. 1997; 11: 337-340./li>
- Choi JW, Kim TK, Kim KW, et al. Anatomic variation in intrahepatic bile ducts: An analysis of intraoperative cholangiograms in 300 consecutive donors for living donor liver transplantation. Korean J Radiol. 2003; 4: 85-90. 10.3348/kjr.2003.4.2.85
- Macdonald DB, Haider MA, Khalili K, et al. Relationship between vascular and biliary anatomy in living liver donors. AJR. 2005; 185: 247-252. 10.2214/ajr.185.1.01850247
- Michels NA. Newer anatomy of the liver and its variant blood supply and collateral circulation. Am J Surg. 1966; 112: 337-347. 10.1016/0002-9610(66)90201-7
- Taghavi SA, Niknam R, Alavi SE, Ejtehadi F, Sivandzadeh GR, et al. Anatomical Variations of the Biliary Tree Found with Endoscopic Retrograde Cholagiopancreatography in a Referral Center in Southern Iran. Middle East J Dig Dis. 2017; 9: 201-205. 10.15171/mejdd.2017.74
- Coco D, Leanza S. Celiac Trunk and Hepatic Artery Variants in Pancreatic and Liver Resection Anatomy and Implications in Surgical Practice. Open Access Maced J Med Sci. 2019; 7: 2563-2568. 10.3889/oamjms.2019.328.
- Arnold M, Abnet CC, Neale RE, Vignat J, Giovannucci EL, et al. Global Burden of 5 Major Types of Gastrointestinal Cancer. Gastroenterology. 2020; 159: 335-349. 10.1053/j.gastro.2020.02.068
- Gunasekaran G, Bekki Y, Lourdusamy V. Surgical Treatments of Hepatobiliary Cancers. Hepatology. 2021; 73: 128-136. 10.1002/hep.31325
- Llovet JM, Montal R, Sia D, Finn RS. Molecular therapies and precision medicine for hepatocellular carcinoma. Nat Rev Clin Oncol. 2018; 15: 599-616.
- Riall TS, Lillemoe KD. Underutilization of surgical resection in patients with localized pancreatic cancer. Ann Surg. 2007; 246: 181-182. 10.1097/SLA.0b013e31811eaa2c
- Griffin JF, Poruk KE, Wolfgang CL. Pancreatic cancer surgery: Past, present, and future. Chin J Cancer Res. 2015; 27: 332-348. 10.3978/j.issn.1000-9604.2015.06.07
- Ushijima T, Sasako M: Focus on gastric cancer. Cancer Cell. 2004; 5: 121-125.
- Michalski CW, Liu B, Heckler M, et al. Underutilization of Surgery in Periampullary Cancer Treatment. J Gastrointest Surg. 2019; 23: 959-965.
- Sameer H, Patel MD. Underutilization of Lymphadenectomy for Gallbladder Cancer: A Persistent Problem with Dire Consequences. Ann. Surg. Oncol. 2021; 28: 2928-2930.
- Saba L, Mallarini G. Anatomic variations of arterial liver vascularization: An analysis by using MDCTA. Surg Radiol Anat. 2011; 33: 559-568.
- Schirmer WJ, Rossi RL, Hughes KS, Munson JL, Braasch JW. Common operative problems in hepatobiliary surgery. Surg Clin North Am. 1991; 71: 1363-89. 10.1016/S0039-6109(16)45595-7
- Setia MS. Methodology Series Module 3: Cross-sectional Studies. Indian J Dermatol. 2016; 61: 261-4. 10.4103/0019-5154.182410.
- Choi TW, Chung JW, Kim HC, Lee M, Choi JW, et al. Anatomic Variations of the Hepatic Artery in 5625 Patients. Radiol Cardiothorac Imaging. 2021, 3:210007. 10.1148/ryct.2021210007
- Pallavi, Ravichandra V. An evaluation of variations of the right hepatic artery using multi detector computed tomography (MDCT). Int J Anat Res. 2016; 4: 3122-3128.
- Poluri K, Agarwal SK, Bansal RP. Hepatic Arterial System- A Radio anatomical Analysis with Multidetector Computed Tomography. Ann. Int. Med. Den. Res. 2018; 4: 22-25.
- Achantani YK, Raju NP, Kumar RR. Variants of Coeliac Trunk, Hepatic Artery and Renal Arteries in Puducherry Population. International. Journal of Anatomy, Radiology and Surgery. 2018; 7: 38-43.
- Abdelkareem H, Ali R, Jibrini M, et al. A study of the anatomic variations of the pancreatico-biliary system in Palestine: a national study. Int Surg J. 2019; 6: 1020-8. 10.18203/2349-2902.isj20191066
- Sambath P, Padmanabhan E, Amirthalligam U, et al. Hepatic Artery and Portal Vein Variations using Contrast Enhanced Computed Tomography Abdominal Angiography. 2022; 11: 20-24.
- Zaki SM, Abdelmaksoud AHK, Khaled BEA, Abdel Kader IA. Anatomical variations of hepatic artery using the multidetector computed tomography angiography. Folia Morphol (Warsz). 2020; 79(2): 247-254.