
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Fertility preservation of infected postpartum uterine dehiscence following cesarean section at Abdulla Mzee Hospital, Tanzania?
radiologiFatma S Mohammed1; Rashid S Hemed2; Khamis Suleiman3; Hidaya A Said1; Yan Ding4*
1Department of Obstetrics and Gynecology, Abdulla Mzee Hospital, Pemba, Zanzibar P.O. Box 193, Pemba, Tanzania.
2Department of Pediatrics, Abdulla Mzee Hospital, Pemba, Zanzibar, P.O. Box 193, Pemba, Tanzania.
3Department of Radiology, Abdulla Mzee Hospital, Pemba, Zanzibar, P.O. Box 193, Pemba, Tanzania.
4Department of Obstetrics and Gynecology, Hospital of Yangzhou University, Yangzhou 225001, China.
*Corresponding Author : Yan Ding
Department of Obstetrics and Gynecology, Hospital of Yangzhou University, Yangzhou 225001, China.
Email: dingyan@yzu.edu.cn
Received : May 13, 2024
Accepted : May 31, 2024
Published : Jun 07, 2024
Archived : www.jcimcr.org
Copyright : © Ding Y (2024).
Abstract
Background: Cesarean section is a crucial part of birth care that may save lives, but it can also perform unintended consequences, they include sepsis, hematoma, uterine dehiscence, and post-cesarean wound infection. These consequences can be diagnosis by radiological examinations such as Computed Tomography (CT), magnetic resonance imaging and ultrasonography. Healing can be aided by broad-spectrum antibiotics utilized during surgery or conservative care. We report a case of uterine dehiscent, identified by CT on eight days after cesarean surgery, which was treated conservatively with subsequent appointments and resulted in positive maternal outcome.
Case presentation: A referral case involving a 27-year-old primiparous lady who was induced into labor at 41 weeks. The pregnancy progressed normally, and the patient had no significant medical or surgical history. After 11 hours of labor, a prolonged labor due to cervical dystocia was diagnosed. One hour later, a transverse lower segment Caesarian Section (CS ) was performed due to labor failing to advance. The uterine incision was closed in two layers with size 2 chromic catgut. Hemostatic sutures were put at the incision’s angles. And three days later, discharged at home.
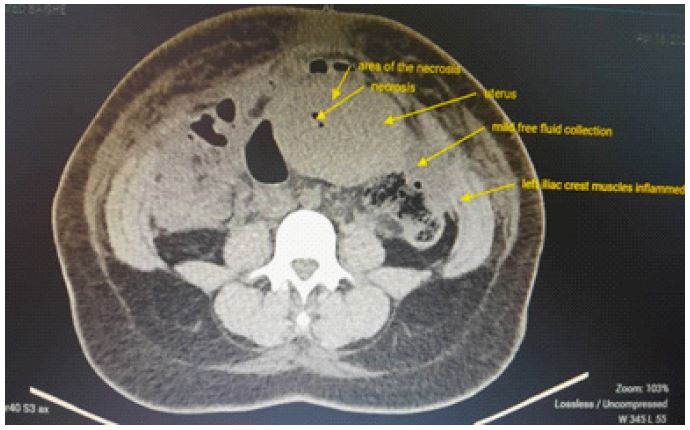
Unfortunately, 10 days after her CS, she was readmitted and referred to our facility. She was examined and reported fever, abdominal pain with distention, and purulent discharge from the incision site and vagina area. The patient’s overall health was unstable, but there was no active bleeding in the vagina. The incision line had an unpleasant discharge. The uterus did not involute at that time, the uterine floor was located above the navel, and the entire abdomen was swollen, with positive tenderness and rebound pain. The CT scan revealed a dehiscence in the lower uterine segment near the uterine scar, with fluid inside. Although both ovaries appeared normal, the intestine was edematous. There was free fluid in the pouch of Douglas (Figure 1).
The laboratory findings were normal. The septic wound in the Pfennestriel incision was treated with antiseptic and normal saline twice a day; one drainage was inserted into the uterine cavity via internal os, with another drainage kept in the posterior fornix using radiologimulcal aids. In these two drainages, normal saline with metronidazole was used for daily lavage. For the first, three days patient was kept on ceftriaxone and metronidazole, she still had a fever and no improvement in abdominal signs. The rechecked white blood cell count is significantly higher than normal. Therefore, upgraded antibiotics to vancomycin and metronidazole for three days, and the clinical symptoms improved significantly.
Under appropriate monitoring, the patient’s sepsis resolved and the drainage was removed after one week. After two weeks, follow-up by clinical parameters and a CT scan showed that the uterine incision had healed well and the restoration was still acceptable. The abdominal incision was given a second suture. Three weeks later, the patient was discharged, and after six months of follow-up, the patient’s intestines showed reduced edema and obliterated dehiscence (Figure 2).
This is a rare report of Fertility preservation of Infected Postpartum Uterine Dehiscence after Cesarean Section in low-resource settings.
Conclusion: In locations with limited resources, especially for women who have a strong desire to have children, the safe option of retaining fertility through Infected Postpartum Uterine Dehiscence following Cesarean Section may be taken into consideration.
Keywords: Cesarean section; Conservative treatment; Computed tomography; Uterine dehiscence; Fertility-preservation; Resource-limited setup.
Citation: Mohammed FS, Hemed RS, Suleiman K, Said HA, Ding Y. Fertility preservation of infected postpartum uterine dehiscence following cesarean section at Abdulla Mzee Hospital, Tanzania. J Clin Images Med Case Rep. 2024; 5(6): 3103.

Discussion
The complications linked to cesarean section have increased exponentially as their prevalence has increased globally. Many reports have been made of complications that range from moderate puerperal infections to endometritis, wound disruption, thrombophlebitis, persistent pelvic pain, adhesions, dehiscence of the uterine scar, and placental abnormalities [1].
Postpartum uterine dehiscence is the opening of the incision line after cesarean section. It is a rare clinical condition and It is an uncommon clinical disease whose incidence ranges from 0.2-1.5% after a low transverse incision to roughly 4-9% after a classical incision [2]. A hematoma on the uterine incision line, diabetes, emergency surgery, infection, surgical technique, multiparous, and an incision made too low in the lower uterine segment or too close to the cervix relatively avascular tissue are among the documented risk factors. Necrosis of the wound’s angles occurs more frequently in these situations [3].
The uterine wall’s weakest point, usually in the cesarean incision, may become necrotic or healthy during a dehiscence. This is thought to be caused by a severe infection that spreads throughout the endometrial and myometrium layers of the uterus. Additionally, postpartum uterine dehiscence may be predisposed by ischemia necrosis of the myometrium brought on by incorrect closure procedures [4].
In the early postpartum period, the opening of the uterine incision may be related to heavy postpartum bleeding [2]. Infection and protracted labor may have exacerbated the wounds infection in the case at hand. It is also possible that surgical methods of our case may create a uterine hematoma, which may lead to a subclinical infection and subsequent tissue necrosis.
While we can attempt conservative management as we did in our case, direct laparotomy is recommended in cases of uterine dehiscence with fulminating infection because this creates an opening between the uterine cavity and the abdominal cavity, which makes it possible for any infection to spread to the abdominal cavity. As a result, patients undergoing conservative treatment should begin a broad-spectrum antibiotic therapy. The majority of patients presented with complaints of pelvic pain and suprapubic sensitivity due to endometritis.
The diagnosis of uterine dehiscence can be made using imaging methods such as CT scan, magnetic resonance imaging, and ultrasound. A full-thickness hypo echoic region with fluid in the uterine incision line will be visible at the site of the uterine incision on ultrasonography. Furthermore, even though Doppler ultrasonography without flow may rule out arteriovenous malformations and hematoma [2].
Patients who have previously experienced uterine dehiscence can have excellent results in subsequent pregnancies if they are managed in a standardized fashion, which includes cesarean delivery before the commencement of labor or promptly at the onset of spontaneous preterm labor. These patients are suggested for a cesarean procedure in the next pregnancy due to poor scar healing and a high incidence of rupture [5].
Conclusion
Conservative care of postpartum uterine dehiscence is a safe and successful therapeutic option for women seeking fertility; however, proper patient screening, shared decision making, and comprehensive informed consent can help to improve desired outcomes.
Declarations
Patient’s perspective: The care provided was timely with a full explanation of the diagnosis and prognosis and a follow-up plan explained.
Acknowledgments: We are humbly grateful for the support and encouragement given by the Obstetrics/gynecology, pediatric and radiology departments at Abdulla Mzee Hospital.
Timeline: The patient was consulted in our hospital and management was initiated. The intervention was done, and the patient was admitted for 3 weeks for conservative management of postpartum uterine dehiscence. Preparation and completion of the case took six months.
Author’s contribution: coauthors contributed to the management of the patient and the writing of the case report. All authors read and approved the final manuscript.
Funding: The cost of preparing this manuscript was covered by the Authors.
Ethical approval and consent to participate: Written informed consent was obtained from the patient for publication of this case report.
Consent for publication: Written informed consent was obtained from the patient for publication of this case and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. A copy of the clearance document is also available for review by the Editor-in-Chief of this journal.
Competing interests: The authors declare that they have no competing interests.
References
- Duff P, Mayer AR. Abdominopelvic abscess resulting from delayed postapartum uterine rupture. American Journal of Obstetrics and Gynecology. 1981; 140(6): 711-3.
- Has R, Topuz S, Kalelioglu I, Tagrikulu D. Imaging features of postpartum uterine rupture: a case report. Abdominal imaging. 2008; 33: 101-3.
- Ida A, Kubota Y, Nosaka M, Ito K, Kato H, Tsuji Y. Successful management of a cesarean scar defect with dehiscence of the uterine incision by using wound lavage. Case Reports in Obstetrics and Gynecology. 2014; 2014.
- Jinturkar D, Sanap D. Post-caesarean surgical site infections: case series of two cases. Int J Clin Obstet Gynaecol. 2019; 3(5): 298-301.
- Fox NS, Gerber RS, Mourad M, Saltzman DH, Klauser CK, Gupta S, et al. Pregnancy outcomes in patients with prior uterine rupture or dehiscence. Obstetrics & Gynecology. 2014; 123(4): 785-9.