
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Myxedema coma with pancytopenia and cardiac dysfunction in young male
Mamta Saini1*; Dayaram2; Arun Kalra3; Trivendra2; Aayushi Dadhich2
1Department of Geriatric Medicine, S.N. Superspeciality Hospital, Sriganganagar, Rajasthan, India.
2Department of Critical Care Medicine, S.N. Superspeciality Hospital, Sriganganagar, Rajasthan, India.
3Department of General Medicine, S.N. Superspeciality Hospital, Sriganganagar, Rajasthan, India.
*Corresponding Author : Mamta Saini
Department of Geriatric Medicine, S.N. Superspeciality Hospital, Sriganganagar, Rajasthan, India.
Email: mamtaaiims18@gmail.com
ORCID ID: 0000-0002-7335-8359
Received : May 16, 2024
Accepted : Jun 03, 2024
Published : Jun 10, 2024
Archived : www.jcimcr.org
Copyright : © Saini M (2024).
Abstract
Myxoedema coma is a critical and potentially fatal condition occurring in untreated or undetected hypothyroidism. It is characterized by systemic organ failure and deteriorating cognitive function. This report outlines a case involving a young male presenting with disturbed consciousness, lowered body temperature, and slow heart rate. Diagnostic tests revealed profound hypothyroidism with significantly elevated Thyroid-Stimulating Hormone (TSH) levels at 83.5 u IU/ml [0.30-4.50], reduced Triiodothyronine (T3) at 0.397 ng/ml [0.69-2.15], and low thyroxine (T4) at 0.793 ug/dl [5.2-12.7], alongside critical cardiac impairment [Ejection fraction=15-20%] and bradycardia accompanied by pancytopenia. The patient required intubation and mechanical ventilation, was fitted with a temporary pacemaker, and received thyroxine replacement and intravenous hydrocortisone. Subsequent complications included fresh bleeding from the endotracheal tube, managed through embolization of the right bronchial artery and additional supportive treatments. Myxoedema should be considered in differential diagnoses for patients exhibiting mental disorientation, hypothermia, and signs of hematologic and cardiac dysfunction. Immediate diagnosis and comprehensive, aggressive treatment across multiple medical specialties are crucial for survival.
Keywords: Hypothyroidism; Myxoedema; Pancytopenia; Cardiac dysfunction; Young male.
Citation: Saini M, Dayaram, Kalra A, Trivendra, Dadhich A. Myxedema coma with pancytopenia and cardiac dysfunction in young male. J Clin Images Med Case Rep. 2024; 5(6): 3107.
Introduction
Myxoedema coma, though termed such, does not necessarily involve coma; it is a critical endocrine emergency with a mortality rate of 50%-60% [1]. This condition is often misnamed since not all affected individuals are comatose, with many only presenting with diminished awareness [2]. It should be suspected in patients who arrive at the Emergency Department exhibiting altered mental states combined with hypothermia and bradycardia, alongside other symptoms such as hypotension, hypoglycemia, and identifiable triggering factors. These triggers can include infections, acute coronary syndrome, cerebrovascular incidents, exacerbations of heart failure, the usage of sedative medications, trauma, and disturbances in electrolytes. Prompt recognition and vigorous treatment are essential to reduce the risk of mortality. This report details a case involving a young male who presented with altered mental status, hypothermia, and pancytopenia.
Case history
A 30-year-old male with intellectual disability since birth (no other previous comorbidity), was brought to our hospital with altered sensorium for the last 7-8 days. The patient was initially treated outside for pancytopenia with altered sensorium where he was also transfused two unit-packed RBCs. His condition declined, prompting a referral to our hospital for advanced diagnostics and management.
Upon presenting to our institution’s emergency department, the patient was drowsy and in altered sensorium with the cooled periphery and hypothermia [temp=94◦F], pulse was 30/min and systolic blood pressure was 70 mmHg.
Electrocardiographic findings were suggestive of complete heart block, arterial blood gas analysis [pH=7.32, PCO2=52, PO2=53, HCO3=26, Na=138, K=3.8], 2-D echocardiography revealed dilated cardiomyopathy with an ejection fraction of 15-20% and concurrent bradycardia was present. Because of severe bradycardia a Temporary Pacemaker Implantation [TPI] was performed.
The patient was shifted to the ICU for further management. On further evaluation TSH=83.5 uIU/ml [0.30-4.50], T3=0.397 ng/ml [0.69-2.15], T4=0.793 ug/dl [5.2-12.7] with pancytopenia (Table 1). The patient was started on intravenous hydrocortisone and Tab Thyroxine 500 mcg was given [through nasogastric tube] along with IV antibiotic and vasopressor support and other supportive treatment. The patient’s sensorium was worsening and the vasopressor requirement was increasing so he was put on mechanical ventilation on the same day.
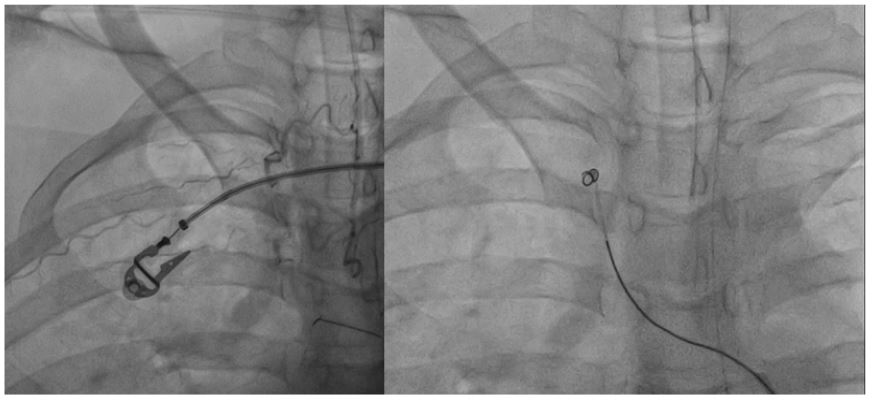
On the second day of admission, the patient’s vasopressor support increased, kidney function worsened, and TLC count in increased. The patient was started on tab triiodothyronine on the third day of hospitalization as this medicine was being brought from another city. On Day four, the patient’s tracheal tube showed active bleeding for which RBC and platelets were transfused, and other supportive treatment was given. Persistent and increasing tracheal bleeding even after transfusion, paved the way for a bronchoscopy, which was performed on day 5th of the admission. Bronchoscopy revealed active bleeding from the right upper anterior and posterior segment bronchus (Figure 1). Afterward, the patient was shifted cath lab and bronchial angiography and rt bronchial artery embolization were done on the same day (Figure 2).
The patient’s sensorium was gradually improving from the 3rd day of admission, the bleeding stopped after embolization, and inotrope support was tapered and stopped. On the 6th day of admission, the patient was extubated. Meanwhile, the TPI was also removed and a repeat 2-d echo showed an improving ejection fraction [45%].
Pancytopenia was persistent for which a bone marrow aspiration was performed, which revealed hypocellular marrow consistent with the myxedema diagnosis. The patient was continued on thyroxine supplementation. The patient was discharged on day 10th of hospitalization with a hemodynamically stable condition and pancytopenia was improving. On the follow-up visit after two months patient is doing very well, his pancytopenia is completely resolved and his thyroid profile is improving. The patient is now on follow-up with an endocrinologist.
Table 1: Laboratory parameters of the patient during hospital stay.
| Parameters (Unit) | Normal range | Day 1 | Day 3 | Day 5 | Day 7 | Day 9 |
|---|---|---|---|---|---|---|
| Haemoglobin (gm/dl) | 13-17 | 11.23 | 6.33 | 5.98 | 7.7 | 9.25 |
| WBC (ths/ul) | 4-10 | 3.27 | 11.140 | 6.66 | 20.490 | 20.11 |
| Platelet count (*103/u L) | 150-410 | 10.3 | 6.0 | 22.0 | 26.3 | 37.0 |
| Urea (mg/dl) | 5-45 | 97.8 | 111.4 | 79.1 | 56.5 | 35.1 |
| Creatinine (mg/dl) | 0.6-1.4 | 0.82 | 1.59 | 1.16 | 1.01 | 0.62 |
| Na (mmol/L) | 137-145 | 139.30 | 140.9 | 142.40 | 145 | 140.70 |
| K (mmol/L) | 3.5-5.1 | 3.79 | 3.43 | 3.30 | 3.01 | 3.40 |
| SGOT (U/L) | 5-37 | 257.6 | 79.9 | |||
| SGPT (U/L) | 5-40 | 155.8 | 55.8 | |||
| Albumin (g/dl) | 3.5-5 | 2.99 | 2.77 | |||
| ALP (U/L) | 45-115 | 324 | 184 | |||
| TSH uIU/ml | 0.30-4.50 | 83.5 | 33 uIU/ml [0.30-4.50] | |||
| T3 ng/ml | 0.69-2.15 | 0.397 | 1.95 [Ft3] pg/ml [2.0-4.2] | |||
| T4 ug/dl | 5.2-12.7 | 0.793 | 9.2 [Ft4] pg/ml [8.9-17.2] |

Discussion
Hypothyroidism can cause anaemia which is most commonly normocytic. Pancytopenia is noted in literature with extreme forms of hypothyroidism in myxoedema coma and all the case reports were in female patients [3,4]. Our case of myxoedema with pancytopenia is a young male patient.
The pathogenesis of the anemia in hypothyroidism is explained as a physiological adaptation to the decreased tissue oxygen requirements resulting from the decrease in the basal metabolic rate. These changes lead to reduced erythropoietic activity of bone marrow [5]. Pancytopenia is generally not seen in hypothyroidism but could be found in Myxoedema. Pancytopenia could be explained by marrow hypoplasia or an associated autoimmune reaction against bone marrow in myxoedema coma [6,7]. In our case, bone marrow aspiration was also done, suggesting hypocellular bone marrow only.
Cardiovascular features can include bradycardia, hypotension, cardiomegaly, low cardiac output, pericardial effusion, cardiogenic shock, ECG changes including non-specific, bundle branch block, and arrhythmias in myxoedema [2]. Severe hypothyroidism leads to cardiac manifestation through multiple mechanisms (a) Hypothyroid state reduces muscle energy production leading to muscle cell injury (b) increased oxidative stress (c) systolic and diastolic dysfunction due to the reduction of sarcoplasmic/endoplasmic reticulum Ca2+- ATPase (SERCA)-2a and α-myosin heavy chain in the severe hypothyroid heart [8,10]. These cardiac manifestations can be reversed with aggressive management including thyroxine supplementation and other supportive measures [11,13].
The patient’s clinical condition gradually improved with aggressive management and appropriate treatment. Thyroid hormone replacement therapy led to the resolution of myxedema coma symptoms, including mental status improvement and normalization of body temperature. The pancytopenia also resolved over time, and cardiac function gradually improved. The patient was discharged with close follow-up and a plan for long-term thyroid hormone replacement therapy.
Conclusion
This rare case report highlights the importance of recognizing and promptly managing myxedema coma, a life-threatening condition. The coexistence of pancytopenia and cardiac dysfunction in this case further emphasizes the complexity of this condition and the need for a comprehensive diagnostic approach. Early diagnosis and appropriate treatment are crucial to improve patient outcomes and prevent potentially fatal complications associated with myxedema coma. Healthcare providers should maintain a high index of suspicion for this rare condition, presenting altered mental status, hypothermia, and multi-system involvement.
Declarations
Author contributions: Mamta Saini: Writing -original draft, writing- review and editing. Dayaram: Review and editing. Arun Kalra: Supervision and review. Trivendra: Review and editing. Aayushi Dadhich: Review and editing.
Funding information: No source of funding for this case report.
Conflict of interest statement: The authors have no conflicts of interest.
Consent: Written informed consent was obtained from the patient’s relative to publish this report by the journal’s patient consent policy.
References
- Wartofsky L. Myxedema Coma. Endocrinol Metab Clin North Am. 2006; 35(4): 687-98.
- Mathew V, Misgar RA, Ghosh S, Mukhopadhyay P, Roychowdhury P, Pandit K, et al. Myxedema Coma: A New Look into an Old Crisis. J Thyroid Res. 2011; 2011: 493462
- Mupamombe CT, Reyes FM, Laskar DB, Gorga J. Myxedema Coma Complicated by Pancytopenia. Case Rep Med. 2019; 2019: 2320751.
- Bulut A, AlSibai K, Norman C. Pancytopenia in a Patient with Severe Hypothyroidism: A Case Report. J Endocr Soc. 2021; 5(1): A946-7.
- DAS KC, MUKHERJEE M, SARKAR TK, DASH RJ, RASTOGI GK. Erythropoiesis and Erythropoietin in Hypo- and Hyperthyroidism. J Clin Endocrinol Metab. 1975; 40(2): 211-20.
- Song SH, McCallum CJ, Campbell IW. Hypoplastic Anaemia Complicating Myxoedema Coma. Scott Med J. 1998; 43(5): 149-50.
- Francis DA. Pure red-cell aplasia: association with systemic lupus erythematosus and primary autoimmune hypothyroidism. BMJ. 1982; 284(6309): 85-85.
- Biron R, Burger A, Chinet A, Clausen T, Dubois-Ferrière R. Thyroid hormones and the energetics of active sodium-potassium transport in mammalian skeletal muscles. J Physiol. 1979; 297(0): 47-60.
- Sarandöl E, Taş S, Dirican M, Serdar Z. Oxidative stress and serum paraoxonase activity in experimental hypothyroidism: effect of vitamin E supplementation. Cell Biochem Funct. 2005; 23(1): 1-8.
- Tang YD, Kuzman JA, Said S, Anderson BE, Wang X, Gerdes AM. Low thyroid function leads to cardiac atrophy with chamber dilatation, impaired myocardial blood flow, loss of arterioles, and severe systolic dysfunction. Circulation. 2005; 112(20): 3122-30.
- Dhakal P, Pant M, Acharya PS, Dahal S, Bhatt VR. Myxedema Coma with Reversible Cardiopulmonary Failure: a Rare Entity in 21St Century. Mædica. 2015; 10(3): 268-71.
- Kousa O, Mansour M, Awad D, Essa A, Qasim A, Sharma A, et al. Reversible bradycardia secondary to myxedema coma: case-report. Rev Cardiovasc Med. 2020; 21(2): 297-301.
- Moss SM, Nagaraja V, Chia EM. Myxoedema crisis as a cause for reversible complete heart block. J Indian Coll Cardiol. 2017; 7(4): 153-6.