
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Quantitative analysis of patient positioning for panoramic imaging: Mandibular cortical morphology in relation to patient head alignment using AI-based computer assisted diagnosis for panoramic radiography?
Yusaku Miki1; Ichiro Ogura1,2*
1Radiology, The Nippon Dental University Niigata Hospital, 1-8 Hamaura-cho, Chuo-ku, Niigata, Niigata 951-8580, Japan.
2Department of Oral and Maxillofacial Radiology, The Nippon Dental University School of Life Dentistry at Niigata, 1-8 Hamaura-cho, Chuo-ku, Niigata, Niigata 951-8580, Japan.
*Corresponding Author : Ichiro Ogura
Department of Oral and Maxillofacial Radiology, The Nippon Dental University School of Life Dentistry at Niigata, 1-8 Hamaura-cho, Chuo-ku, Niigata, Niigata 951-8580, Japan.
Tel: 81-25-267-1500;
Email: ogura@ngt.ndu.ac.jp
Received : May 22, 2024
Accepted : Jun 05, 2024
Published : Jun 12, 2024
Archived : www.jcimcr.org
Copyright : © Ogura I (2024).
Abstract
Objective: This study aimed to investigate quantitative analysis of patient positioning for panoramic imaging, especially mandibular cortical morphology in relation to patient head alignment using Artificial Intelligence-Based Computer Assisted Diagnosis (AI-CAD) for panoramic radiography.
Methods: A dry skull, such as the setting position of the head shifted 5 mm and 10 mm for right, left, superior, inferior, anterior and posterior from the standard position, was underwent panoramic radiography. The mandibular cortical morphology, such as Mandibular Cortical Index (MCI) and degree of deformation, was analyzed with an AI-CAD. A P value less than 0.05 was considered to indicate statistical significance.
Result: Regarding setting position of the head, the MCI of inferior 5 mm (P=0.008), inferior 10 mm (P=0.048) and posterior 10 mm (P=0.008) were significant differences for standard position. The degree of deformation for the inferior (5 mm: 38.0±2.6 (P=0.008) and 10 mm: 37.0±2.1 (P=0.008)) and posterior (5 mm: 32.6±9.5 (P=0.032) and 10 mm: 43.4±6.0 (P=0.008)) were significantly higher than that of standard position (19.4±4.7). Furthermore, the degree of deformation for the anterior (5 mm: 9.6±5.5 (P=0.016) and 10 mm: 6.6±2.2 (P=0.008)) were significantly lower than that of the standard position.
Conclusion: The AI-CAD could be a useful tool for the quantitative analysis of patient positioning for panoramic imaging.
Keywords: Computer-assisted diagnosis; Panoramic radiography; Patient positioning.
Citation: Miki Y, Ogura I. Quantitative analysis of patient positioning for panoramic imaging: Mandibular cortical morphology in relation to patient head alignment using AI-based computer assisted diagnosis for panoramic radiography. J Clin Images Med Case Rep. 2024; 5(6): 3113.
Introduction
Panoramic radiography is the most common extra-oral radiograph carried out in dentistry. However, errors in panoramic radiography are relatively high with patient positioning, preparation/instruction being the most common cause of error [1]. There are reports of accuracy and head positioning effects on measurements of anterior tooth length using 3-dimensional and conventional panoramic radiography [2].
In the field of dentistry, the morphology of mandibular cortical bone has attracted attention as a predictor of osteoporosis. A previous study proposed a method to detect signs of osteoporosis on panoramic images [3-7]. Two of these studies focused on the morphology of the inner surface of the mandibular cortex below the mental foramen [3,4]. Subsequently, the usefulness of the Mandibular Cortical Index (MCI) as a predictor of osteoporosis has been proven.
Recently, an Artificial Intelligence-Based Computer Assisted Diagnosis (AI-CAD) for panoramic radiography “PanoSCOPE” was developed to scan the inferior margin of the mandible and automatically evaluate mandibular cortical morphology, such as the MCI and degree of deformation, and the AI-CAD system is an effective tool for pre-screening of osteoporosis by panoramic radiography [8-12]. However, no studies were found for the errors in panoramic radiography depending on patient head alignment using the AI-CAD system. This study aimed to investigate quantitative analysis of patient positioning for panoramic imaging, especially mandibular cortical morphology in relation to patient head alignment using AI-CAD for panoramic radiography.
Materials and methods
Used dry skull: This prospective study was approved by the Ethics Committee of The Nippon Dental University School of Life Dentistry at Niigata (ECNG- R-518). A dry skull with no scratches or stains was used in the vicinity of the mental foramen, which is the part to be analyzed. The upper and lower jaws were fixed so that they were in the maximal intercuspal position.
Setting position of the head: A light beam was used to establish the reference when taking radiographs of the dry skull. A midline light beam is located in the median plane. The light beam in the Frankfurt plane is parallel to the ground. The light beam of the fault area is located in the distal part of the canine teeth of the upper and lower jaws. The state in which the above three conditions are met was defined as the “standard position”. Continue to take panoramic images in a state shifted from the standard position.
For the first pattern, the skull was rotated 5 mm and 10 mm left and right around the chin rest from the midline light beam. For the second pattern, the skull was moved upward (superior) and downward (inferior) by 5 mm and 10 mm from the Frankfurt plane based on eye level. For the third pattern, the light beam located at the canine teeth of the upper and lower jaws was moved forward (anterior) and backward (posterior) by 5 mm and 10 mm. Based on our experience, in the case of patients who are difficult to take panoramic images, we assumed that there would be a maximum deviation of approximately 10 mm. A total of 65 shots were taken, 5 times at the standard position and 4 sets of 5 times at the shifted position of 3 patterns. When taking at the same position, the skull was removed once, placed at the same position, and taken again.
Data analysis: Panoramic radiography was performed using Veraviewepocs (MORITA, Kyoto, Japan), following our hospital maxillofacial protocol (a tube voltage; 70 kV, a tube current; 10 mA) [8-12]. CR Console (FUJIFILM, Tokyo, Japan) was used as the medical image processing device. Bone morphology analysis was performed with PanoSCOPE (MEDIA, Tokyo, Japan) using panoramic images at each head position, and the MCI and the thickness of the mandible were calculated, following our institutional protocol [8-12]. The MCI classification was as follows: normal (class 1), mildly to moderately eroded (class 2). Bone thickness was measured in both lower jaws. In addition, the degree of deformation was calculated using the thickness and MCI. It was numeric from 0 to 100, and the closer the number is to 0, the lower the suspicion of osteoporosis.
Statistical analysis: The cortical bone thickness and degree of deformation were performed by Mann-Whitney U-test. MCI classifications were performed by Fisher exact test. Those statistical analyses were evaluated with the statistical package SPSS Statistics (version 26, IBM Japan, Tokyo, Japan) using a 5% significance level.
Results
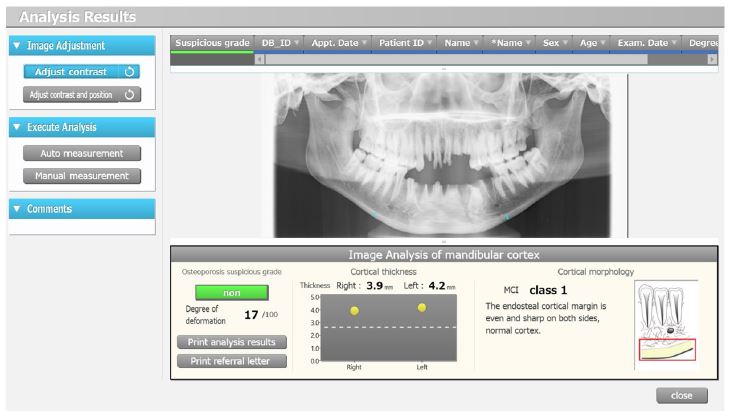
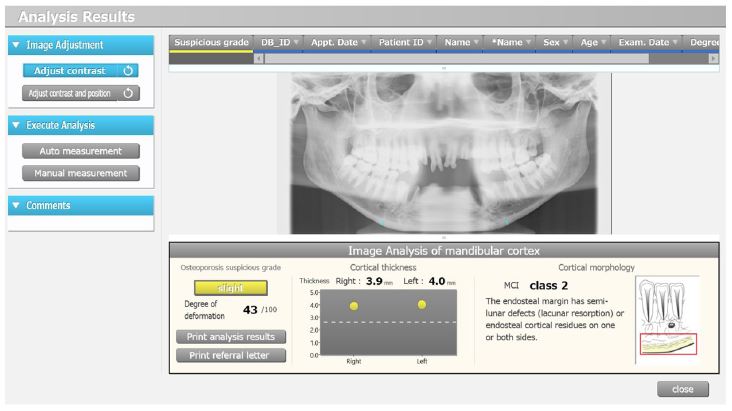
Table 1 shows mandibular cortical morphology in relation to patient head alignment using AI-CAD for panoramic radiography. Regarding setting position of the head, the MCI of inferior 5 mm (P=0.008), inferior 10 mm (P=0.048) and posterior 10 mm (P=0.008) were significant differences for standard position. The degree of deformation for the inferior (5 mm: 38.0±2.6 (P=0.008) and 10 mm: 37.0±2.1 (P=0.008)) and posterior (5 mm: 32.6±9.5 (P=0.032) and 10 mm: 43.4±6.0 (P=0.008)) were significantly higher than that of standard position (19.4±4.7). Furthermore, the degree of deformation for the anterior (5 mm: 9.6±5.5 (P=0.016) and 10 mm: 6.6±2.2 (P=0.008)) were significantly lower than that of standard position (19.4±4.7). Figures 1-3 show PanoSCOPE software of standard position, anterior 10 mm, and posterior 10 mm, respectively.
Table 1: Mandibular cortical morphology in relation to patient head alignment using AI-CAD for panoramic radiography.
| Setting position of the head (n = 5) | Mandibular cortical morphology using AI-basedcomputer assisted diagnosis for panoramic radiography | |||||||
|---|---|---|---|---|---|---|---|---|
| Cortical bone thickness (mm) | MCI(class 1 vsclass 2) | Degree of deformation | ||||||
| Right side | Left side | |||||||
| Mean ± SD | P-value | Mean ± SD | P-value | 1 vs 2 | P-value | Mean ± SD | P-value | |
| Standard position | 3.64 ± 0.29 | ― | 4.64 ± 0.32 | ― | 5 vs 0 | ― | 19.4 ± 4.7 | ― |
| Right side 5 mm | 3.72 ± 0.36 | 0.841 | 3.96 ± 0.32* | 0.016 | 4 vs 1 | 1.000 | 21.0 ± 12.0 | 0.690 |
| Right side 10 mm | 3.40 ± 0.12 | 0.151 | 4.38 ± 0.74 | 0.421 | 5 vs 0 | ― | 14.6 ± 5.6 | 0.310 |
| Left side 5 mm | 3.44 ± 0.15 | 0.548 | 4.40 ± 0.49 | 0.421 | 4 vs 1 | 1.000 | 26.6 ± 10.1 | 0.222 |
| Left side 10 mm | 3.44 ± 0.56 | 0.310 | 4.22 ± 0.51 | 0.222 | 4 vs 1 | 1.000 | 24.2 ± 11.6 | 0.548 |
| Superior 5 mm | 4.02 ± 0.37 | 0.095 | 4.28 ± 0.55 | 0.421 | 5 vs 0 | ― | 18.4 ± 8.4 | 1.000 |
| Superior 10 mm | 3.86 ± 0.50 | 0.690 | 4.18 ± 0.51 | 0.151 | 5 vs 0 | ― | 13.0 ± 3.4 | 0.056 |
| Inferior 5 mm | 3.40 ± 0.00 | 0.151 | 4.28 ± 0.55 | 0.421 | 0 vs 5* | 0.008 | 38.0 ± 2.6* | 0.008 |
| Inferior 10 mm | 3.26 ± 0.32 | 0.151 | 4.18 ± 0.51 | 0.151 | 1 vs 4* | 0.048 | 37.0 ± 2.1* | 0.008 |
| Anterior 5 mm | 3.82 ± 0.26 | 0.548 | 4.32 ± 0.50 | 0.310 | 5 vs 0 | ― | 9.6 ± 5.5* | 0.016 |
| Anterior 10 mm | 3.70 ± 0.17 | 0.421 | 4.34 ± 0.38 | 0.310 | 5 vs 0 | ― | 6.6 ± 2.2* | 0.008 |
| Posterior 5 mm | 3.66 ± 0.24 | 0.841 | 4.34 ± 0.26 | 0.151 | 2 vs 3 | 0.167 | 32.6 ± 9.5* | 0.032 |
| Posterior 10 mm | 3.44 ± 0.34 | 0.222 | 4.38 ± 0.38 | 0.222 | 0 vs 5* | 0.008 | 43.4 ± 6.0* | 0.008 |

Discussion
In panoramic images, objects shrink or expand in size compared to their actual size [13]. Therefore, we expected that the thickness of the mandibular cortical bone would change, but there were no significant changes in the thickness, except for a pattern (right side 5 mm). Head positioning with a 10 mm deviation suggested that no expansion or contraction occurred at around the mental foramen.
On the other hand, in the analysis of MCI and degree of deformation, there were significant differences in the anterior, posterior and inferior positions compared to the standard position. In the backward and downward patterns, the mandibular anterior tooth was blurred. In a previous study, when they moved a simulated human head backward and downward, the anterior tooth of the mandible became blurry in panoramic images [2]. Similarly, in our study, this system incorrectly determined that the cortical bone was rough because the mandibular anterior tooth was blurred. On the other hand, when the position was placed forward, there was a significant difference compared to the standard position in degree of deformation because the anterior tooth of the mandible was clearly visible. This means that the bone was incorrectly determined to be dense.
There is a study that investigated whether the analysis results of PanoSCOPE change when images are taken at different times in the same patient. In this study, PanoSCOPE analysis results did not change between patients before and after dental implant placement [10]. Our study had different results from previous studies because the head was moved significantly from the standard position. This occurs in the case of patients in wheelchairs or elderly people because it is difficult to set the imaging position. Therefore, if the head position is moved from the standard position and photographed, it should not be used for PanoSCOPE analysis. If panoramic images are taken multiple times for the same patient, it is best to select an image in which the area around the mental foramen or the mandibular anterior tooth is not blurred and use it for analysis.
A limitation of this study is that we do not know whether the soft tissue of the head and neck or the hard tissue of the neck influenced the analysis. In addition, the study was conducted for only a dry skull for single patient whose gender, age and other histories were unknown. Patients who have difficulty obtaining panoramic radiography may be unwillingly taken out of the standard position. In the above case, the photographed image with clear mandibular anterior tooth should be used for analysis. In the future, it will be necessary to determine the allowable value for head position deviation.
Conclusion
This pilot study examined the relationship between setting positioning of the head and mandibular cortical morphology using PanoSCOPE. The results indicated that the degree of deformation depend on the setting positioning of the head. The AI-CAD could be a useful tool for the quantitative analysis of patient positioning for panoramic imaging.
Declarations
Acknowledgements: Not applicable.
Conflict of interest: The authors declare that they have no conflict of interest.
Funding statement: This study was not funded.
Ethics approval and consent to participate: The study was approved by the institutional review board of The Nippon Dental University School of Life Dentistry at Niigata (approved no. ECNG- R-518), and informed consent was obtained from all individual participants included in the study. All procedures performed in studies involving human participants were in accordance with the Helsinki declaration as revised in 2013 and its later amendments.
Availability of data and material: Contact the corresponding author for data requests.
References
- Loughlin A, Drage N, Greenall C, Farnell DJJ. An investigation into the impact of acquisition location on error type and rate when undertaking panoramic radiography. Radiography (Lond). 2017; 23: 305-9.
- Kitai N, Murabayashi M, Sugimoto H, Fujiwara A, Tome W, Katsumata A. Accuracy and head positioning effects on measurements of anterior tooth length using 3-demensional and conventional dental panoramic radiography. Am J Orthod Dentofacial Orthop. 2017; 151: 607-15.
- Klemetti E, Kolmakov S, Kroger H. Pantomography in assessment of the osteoporosis risk group. Scand J Dent Res. 1994; 102: 68-72.
- Taguchi A, Tanimoto K, Suei Y, Otani K, Wada T. Oral signs as indicators of possible osteoporosis in elderly women. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 80: 612-6.
- Taguchi A, Suei Y, Ohtsuka M, Otani K, Tanimoto K, Ohtaki M. Usefulness of panoramic radiography in the diagnosis of postmenopausal osteoporosis in women. Width and morphology of inferior cortex of the mandible. Dentomaxillofac Radiol. 1996; 25: 263-7.
- Taguchi A. Triage screening for osteoporosis in dental clinics using panoramic radiographs. Oral Dis. 2010; 16: 316-27.
- Roberts M, Yuan J, Graham J, Jacobs R, Devlin H. Changes in mandibular cortical width measurements with age in men and women. Osteoporos Int. 2011; 22: 1915-25.
- Ogura I, Kobayashi E, Nakahara K, Haga-Tsujimura M, Igarashi K, Katsumata A. Computer programme to assess mandibular cortex morphology in cases of medication-related osteonecrosis of the jaw with osteoporosis or bone metastases. Imaging Sci Dent. 2019; 49: 281-6.
- Ogawa R, Ogura I. AI-based computer-aided diagnosis for panoramic radiographs: quantitative analysis of mandibular cortical morphology in relation to age and gender. J Stomatol Oral Maxillofac Surg. 2022; 123: 383-7.
- Ogawa R, Ogura I. Change in the mandibular cortical morphology at pre and postdental implant operations using artificial intelligence based computer aided diagnosis for panoramic radiography. J Oral Maxillofac Radiol. 2022; 10: 76-9.
- Ogawa R, Ogura I. Quantitative analysis of mandibular cortical morphology using artificial intelligence-based computer assisted diagnosis for panoramic radiography on underlying diseases and dental status in women over 20 years of age. J Dent Sci. 2024; 19: 937-44.
- Ohmori M, Takashio T, Takemoto S, Mori N, Sato S, Tezuka Y, et al. Mandibular cortical morphology in periodontitis patients with stage III/IV using AI-based computer-assisted diagnosis for panoramic radiography. J Clin Images Med Case Rep. 2024; 5: 2959.
- Nikneshan S, Sharafi M, Emadi N. Evaluation of the accuracy of linear and angular measurements on panoramic radiographs taken at different positions. Imaging Sci Dent. 2013; 43: 191-6.