
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Lung abscesses complicating hydrocarbon ingestion in a child: About a rare and unusual case
H Benfadila*; K ElFakiri; S Mghar; N Rada; G Draiss; M Bouskraoui
Pediatric Department, Unit of Pneumology and Allergology, Mother-Child Hospital, Cadi Ayaad University, Marrakech, Morocco.
*Corresponding Author : Hajar Benfadila
Pediatric Department, Unit of Pneumology and Allergology, Mother-Child Hospital, Cadi Ayaad University, Marrakech, Morocco.
Email: hajar.benfadila@gmail.com
Received : May 22, 2024
Accepted : Jun 05, 2024
Published : Jun 12, 2024
Archived : www.jcimcr.org
Copyright : © Benfadila H (2024).
Citation: Benfadila H, ElFakiri K, Mghar S, Rada N, Draiss G, et al. Lung abscesses complicating hydrocarbon ingestion in a child: About a rare and unusual case. J Clin Images Med Case Rep. 2024; 5(6): 3116.
Introduction
Accidental ingestion of hydrocarbon in children is common in developing countries, the main complication of which is chemical pneumonia with deaths occurring in four to ten percent of reported cases. Among various pulmonary complications, pneumatocele is a complication known in the literature unlike the evolution of pneumonia towards an abscess which is considered relatively rare. We report an unusual and rare observation of a pulmonary abscess complicating hydrocarbon ingestion in an 18 month old girl after consent free and enlightened from his parents.
Observation
A girl Z.Z aged 18 months, vaccinated according to the national immunization plan without any particular pathological history, the anamnesis found an accidental ingestion of hydrocarbon 22 days before leading to excitability, disinhibition, behavioral problems and nausea followed by drowsiness evolving into obtundation, she was admitted to the pediatric emergency room and placed under surveillance for 12 hours then returned to normal neurological status. The patient had a fever with a productive cough associated with respiratory distress for 7 days. Admission, the patient was in good general condition, weight at 8 kg (-2DS), height at 70 cm (-2DS), polypneic at 45 cycles/minute, normocardium at 110 beats/minute, O2 saturation at 85 at l ‘free area, feverish at 38.5. This presents signs of respiratory struggles such as under-costal drawing, flapping of the wings of the nose. On pulmonary examination there were no rales on auscultation and we found right basal dullness. The biological assessment revealed hyperleukocytosis at 16,240/ul with a predominance of neutrophils 10,880/ul with lymphocyte at 4010/ul and a CRP at 43 mg/l, a blood culture was sterile. Chest radiography revealed a well-limited non-systematized opacity of excavated water tone on the right and a hydroaeric level on the left (Figure 1).
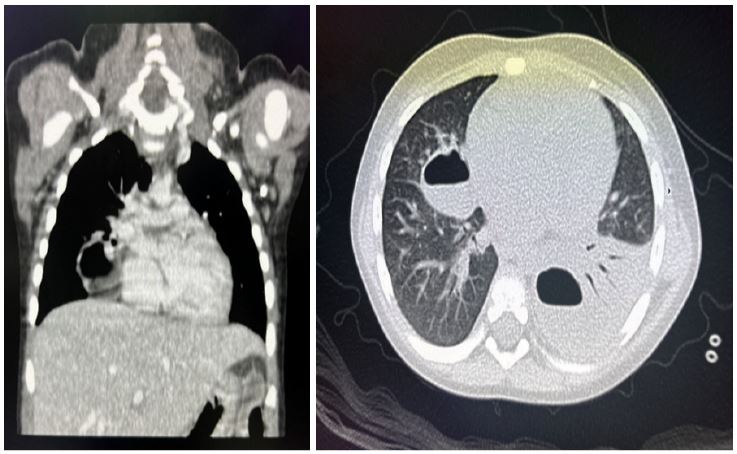
Thoracic CT showed an individualization of a left medio-basal cavitary lesion, with thickened wall, measuring 31x21 mm, site of a hydro-aeric level and drained by segmental branches opposite and embedded in a focus of condensation parenchymatous involving the entire lower left lobe seat of air bronchogram, it is associated with another middle lobar cavity bulging on the large fissure, with thickened and irregular wall in places seat of a hydro-aeric level measuring 27x22 mm, drained by segmental bronchi facing each other. There was a band condensation of the medial segment of the middle lobe, site of air bronchogram (Figure 2). HIV serology was negative and an assessment of the immune deficiency in particular the weight dosage of immunoglobulins IGG at 8.884 g/l, IGM at 1.032 g/l, IGA at 1.19 g/l, IGE at 4.63 was normal was put on ceftriaxone at a dose of 80 mg/kg/day for 17 days intravenously then relayed orally for 8 weeks. The evolution was marked by improvement under treatment with gain of apyrexia one day later then weaned from the oxygen therapy four days later. After a 6-week follow-up, the patient was in good general condition with a follow-up chest X-ray showing partial cleaning of the abscesses.

Discussion
In the literature, lung abscess complicated by hydrocarbon ingestion is very rare in the pediatric population. Lung abscess is a circumscribed, thick-walled lung cavity that contains purulent material resulting from suppuration and necrosis of the involved lung parenchyma [1,2]. There are two main types of pulmonary abscesses in children: primary, in which there are no predisposing factors, or secondary, in which there are underlying predisposing factors, either pulmonary or systemic [1].
Other reported classifications include multilocular and uniloculated, aspirational and hematogenous [3]. In our case we are faced with a secondary lung abscess. Case series of pediatric lung abscesses have reported unwarranted variations in management with alarming prolonged hospitalization [3,4]. The most common clinical signs of lung abscess reported by studies: fever, cough and dyspnea [5,6].
Lung injury results from aspiration during or after ingestion of hydrocarbons. Increased volatility, low viscosity, and decreased surface tension of the ingested substance are linked to an increased risk of aspiration and lung injury because these characteristics make it easier for the hydrocarbon to penetrate the bronchial tree and spread across the bronchial tree. the respiratory mucosa [7,8]. Vomiting, choking, or coughing during or after ingestion increases the risk of aspiration [9]. Hydrocarbons destroy surfactant, cause tissue necrosis, alveolar and interstitial edema and inflammation leading to decreased lung compliance, increased work of breathing and hypoxemia [1,9-12].
The clinical manifestations after ingestion of hydrocarbon are essentially neurological and can vary depending on the specific substance inhaled [11]. Typically, poisoning symptoms progress through a series of stages depending on the amount of inhalation of a particular substance. Each step can be extended by inhaling several times. The first stage is often described as euphoria, followed by excitability, disinhibition and impulsive behavior over 10 minutes [13-18]. The most common symptoms were neurological and included headache, dizziness and nausea. The other most common neurological symptoms were tongue dysesthesia, leg numbness, muscle weakness, tinnitus and blurred vision. The second stage is characterized by CNS depression, such as slurred speech, confusion, hallucinations, diplopia, tremor, ataxic gait, visual changes, and weakness. The final stages are marked by drowsiness evolving into obtundation with the possibility of coma, convulsions and death [13-18].
On the other hand, lung injuries due to hydrocarbons most often occur when young children ingest the liquid and aspirate during or after this event which liquid hydrocarbon is sprayed through the mouth. Although lung damage can occur without the concept of vomiting, which is a risk factor for aspiration. Commonly reported symptoms after aspiration of hydrocarbons are cough, nausea/vomiting, drowsiness, fever, tachycardia [19-21]. Agitation, stupor and convulsions are also reported, wheezing or rales [19,22].
In our patient she presented excitability, disinhibition and a behavioral disorder and nausea followed by drowsiness evolving into obtundation without respiratory signs or fever up to 22 days after ingestion where she presented a fever associated with a cough and respiratory distress, something which is not described in the literature, generally respiratory signs after inhalation appear within the first hours.
Radiological images found in the literature after acute hydrocarbon aspiration generally show bilateral interstitial opacities in the lobes, which are usually located in the middle and lower lobes. Air bronchograms, pneumatocele, and pleural effusions have been reported. The radiological abnormalities can last for months. In our case, the chest x-ray revealed a thick-walled cavitary image at the level of the pulmonary hemi-field on the right, we also visualize a bronchus which opens onto this cavity in the form with a linear clarity with parallel edges creating with the cavity a tennis racket image suggesting a pulmonary abscess and on the left an oval parenchymal hyper clarity surrounded by a thin wall surrounded by alveolar type foci with air bronchograms giving an appearance of pneumatocele which can simulate a pulmonary abscess, which represents a pediatric particularity.
The use of diagnostic tomography is only useful in certain doubtful situations, in particular to differentiate a pulmonary abscess from a bronchogenic cyst in children. This examination will rather be indicated in search of an underlying local cause, or in order to better clarify the anatomical relationships preoperatively [23,24]. A chest CT scan showed a left middle lobar and mid-basal lung abscess, associated with foci of pulmonary condensation. Faced with our situation of bilateral lung abscess requires us to look for an underlying cause. Generally it may be a general cause such as an immune deficiency, a hematological malignancy, Down syndrome or encephalopathy. The predisposing factor may be local, such as a foreign body or bronchopulmonary malformation [25].
The only entry point found is the hydrocarbon ingestion accident, and it is considered to be the predisposing factor despite the rarity of the occurrence of a pulmonary abscess after an hydrocarbon ingestion accident, especially with the notion of appearance of respiratory symptoms after a free interval. The recommended initial treatment for primary or secondary lung abscesses in children is appropriate intravenous antibiotic therapy alone. Medical treatment based on double parenteral bactericidal antibiotic therapy for 4 to 6 weeks targeting Staphylococcus aureus, Streptococcus pneumoniae and Gram-negative bacilli of the upper respiratory tract. An antibiotic active on anaerobes will be combined in patients at risk of aspiration pneumonia. An antifungal will be combined in immunocompromised patients. Respiratory physiotherapy, or better bronchoaspiration, facilitates drainage and reduces long-term after-effects. If initial treatment has failed or was suboptimal, percutaneous aspiration is recommended before proceeding with more invasive procedures.
Surgical drainage with a pigtail catheter is a minimally invasive procedure and the procedure of choice before proceeding with a more invasive procedure. Pediatricians should be alerted to the potential underlying cause, particularly if there has been no optimal response to initial treatments.
Our patient received Ceftriaxone 80 mg/kg/day with Gentamycin 3 mg/kg/day for 3 weeks then relay orally with a treatment duration extended to 8 weeks.
The prognosis of lung abscess remains severe, particularly in cases of secondary PA. Mortality has certainly decreased in recent decades, going from 65% in the 1960s to 8.7% during the last decade. However, pulmonary sequelae such as bronchial dilatation or pulmonary fibrosis still threaten one in six children. According to the literature available to date, there is no convincing evidence for the early administration of steroid or antibiotic prophylaxis to prevent chemical pneumonitis and improve outcomes in all children with acute accidental hydrocarbon poisoning. However, if there are pre-existing risk factors or established pneumonitis and/or secondary infections, steroids and antibiotics could be used therapeutically.
Conclusion
Accidental ingestion of petroleum distillates during childhood may result in aspiration pneumonia depending on the volatility, viscosity, and surface tension of the substance and the occurrence of vomiting. Children with hydrocarbon pneumonia who become symptomatic within 6 to 8 hours have a benign clinical course, which requires monitoring and supportive care, except for cases progressing to acute respiratory distress syndrome. The mortality rate is low, but chemical pneumonia can be complicated by subtle abnormalities in lung function, including lung abscess several days after the initial lung injury.
References
- Choi MS, Chun JH, Leek Rha, Choi YH, SH Clinical features of pediatric lung abscess: 15 years of experience in two university hospitals. Korean J. Pediatr. 2015; 58:478-483.
- Feki W, Ketata W, Bahloul N, Ayadi H, Yangui I, Kammoun S. Lung abscess: diagnosis and management. Rev. Evils. Breathe. 2019; 36:707-719.
- Madhani K, McGrathx E, Guglani L. A 10-year retrospective review of pediatric lung abscesses from a single center. Ann. Thoracic. Med. 2016; 11:191-196.
- Fernando DT, Bhatt R, Saiganesh A, Schultz A, Gera P. Lung abscess: 14 years of experience in a tertiary pediatric hospital. ANZ J. Surg .2022. Early online publication.
- Yen CC, Tang RB, Chen SJ, Chin TW. Pediatric lung abscess: retrospective review of 23 cases.J. Microbiol. Immunol. Infect. 2004; 37:45-49.
- ChanCP, Huang LM, Wu PS, Chang PY, Yang TT, Lu CY, Lee IP, Chen JM, Lee CY, Chang LY. Clinical management and outcome of pulmonary abscess in children: 16 years of experience.J. Microbiol. Immunol. Infect. 2005; 38:183-188.
- Tormoehlen LM, Tekulve KJ, Nanagas KA. Hydrocarbon toxicity: a review. Clin Toxicol (Phila). 2014; 52:479-489.
- Cobaugh DJ, Seger DL, Krenzelok EP. Hydrocarbon toxicity: an analysis of AAPCC TESS data. Przegl Lek. 2007; 64:194-196.
- Victoria MS, Nangia BS. Hydrocarbon poisoning: an assessment. PediatrEmerg Car.e 1987; 3:184-186.
- Sen V, Kelekci S, Selimoglu Sen H, Yolbas I, Gunes A, Abakay O, FuatGurkan M. An evaluation of cases of pneumonia occurring following hydrocarbon exposure in children. EurRev Med PharmacolSci. 2013; 17:9-12.
- Sen V, Kelekci S, Selimoglu Sen H, Yolbas I, Gunes A, Abakay O, FuatGurkan M. An evaluation of cases of pneumonia occurring following hydrocarbon exposure in children. EurRev Med PharmacolSci. 2013; 17:9.
- Schneider S, Schurch D, Geiser M. Aspiration toxicology of hydrocarbons and lamp oils studied by in vitro technology. ToxicolIn Vitro. 2013; 27:1089-1101.
- Brook MP, McCarron MM, Mueller JA. Ingestion of pine oil cleanser. Ann Emerg Med. 1989; 18:391-395.
- Lifshitz M, Sofer S, Gorodischer R. Hydrocarbon poisoning in children: a 5-year retrospective study. Wilderness Environ Med. 2003; 14:78-82.
- Anas N, Namasonthi V, Ginsburg CM. Criteria for hospitalization of children who have ingested products containing hydrocarbons. JAMA. nineteen eighty one; 246:840-843.
- Truemper E, Reyes de la Rocha S, Atkinson SD. Clinical characteristics, pathophysiology and management of hydrocarbon ingestion: case report and review of the literature. PediatrEmerg Care. 1987; 3:187-193.
- Scalzo AJ, Weber TR, Jaeger RW, Connors RH, Thompson MW. Extracorporeal membrane oxygenation for hydrocarbon aspiration. Am J Dis Child. 1990; 144:867-871.
- American Academy of Neurology, Editor Clinical Practice Guidelines Process Manual. St. Paul, MN: American Academy of Neurology. 2011.
- Cobaugh DJ, Seger DL, Krenzelok EP. Hydrocarbon toxicity: an analysis of AAPCC TESS data. Przegl Lek. 2007; 64:194-196.
- Sen V, Kelekci S, Selimoglu Sen H, Yolbas I, Gunes A, Abakay O, FuatGurkan M. An evaluation of cases of pneumonia occurring following hydrocarbon exposure in children. EurRev Med PharmacolSci. 2013; 17:9-12.
- Van Gorcum TF, Hunault CC, Van Zoelen GA, De Vries I, Meulenbelt J. Lamp oil poisoning: has the European directive reduced the number and severity of poisonings? J Toxicol Clin Toxicol. 2009; 47:29-34.
- Lifshitz M, Sofer S, Gorodischer R. Hydrocarbon poisoning in children: a 5-year retrospective study. Wilderness Environ Med. 2003; 14:78-82.
- WHO Emro Pediatric Hydrocarbon Study Group CE, Bond GR, Pieche S, Sonicki Z, Gamaluddin H, El Guindi M, Sakr M, et al. A clinical decision rule for the triage of children under 5 years of age with hydrocarbon (kerosene) aspiration in developing countries. J-Toxicol Clin Toxicol. 2008; 46:222-229.
- Johnson JF, Shiels WE, White CB, Williams BD. Concealed pulmonary abscess: diagnosis by computed tomography. Pediatrics. 1986; 78:283-6.
- Stark DD, Federle MP, Goodman PC, Podrasky AE, Webb WR. Differentiating lung abscess and empyema: radiography and computed tomography. Am J Roentgenol. 1983; 141:163-7.
- Chen-Chein Y, Ren-Bin T, Shu-Jen C, Tai-Wai C. Pediatric lung disease: a retrospective review of 23 cases. J MicrobiolImmunol Infect. 2004; 37:45-9.