
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Sudden sensorineural hearing loss and vertigo due to inner ear hemorrhage: A case report
Sameh Mezri*; Mariem Selmi
ENT Department, Military Hospital of Tunis, University El Manar, Tunisia.
*Corresponding Author : Sameh Mezri
ENT Department, Military Hospital of Tunis, University El Manar, Tunisia.
Email: samehmezri@yahoo.fr
Received : May 22, 2024
Accepted : Jun 06, 2024
Published : Jun 13, 2024
Archived : www.jcimcr.org
Copyright : © Mezri S (2024).
Abstract
Sudden deafness is a common cause of emergency consultations in otology. Usually, despite investigation, no aetiology is known. Intra-cochlear haemorrhage, is a rare cause of Sudden Sensorineural Hearing Loss (SSNHL) and may be associated with various labyrinthine disorders. In these cases, Magnetic Resonance Imaging (MRI) is the clef of diagnosis. We report a case of a 70-year-old patient who is referred to our department for left sudden hearing loss, tinnitus and vertigo. Otoscopic and neurological examination were normal and pure tone audiometry indicated left profound sensorineural hearing loss. Videonystagmography (VNG) revealed a left vestibular deficit. MRI performed demonstrated a high signal intensity inside the cochlea on unenhanced T1-weighted images, no other abnormalities were found, in particular no enhancement after intravenous administration of gadolinium. No etiology has been identified. The vertigo disappeared rapidly under corticosteroid treatment and hyperbaric oxygen therapy, but the hearing did not improve. The finding of an intra-labyrinthine hemorrhage causing SSNHL is rare and hearing prognosis is poor.
Keywords: Inner ear; Hemorrhage; Sudden hearing loss; Magnetic resonance imaging.
Citation: Mezri S, Selmi M. Sudden sensorineural hearing loss and vertigo due to inner ear hemorrhage: A case report. J Clin Images Med Case Rep. 2024; 5(6): 3118.
Introduction
Sudden Sensorineural Hearing Loss (SSNHL) is defined as a hearing loss of more than 30 dB in at least three contiguous frequencies occurring in a period of less than 72 hours [1]. Investigation of SSNHL require audiological exam and MRI [2]. It is often classified as idiopathic, although several causes have been suggested, including viral infections, immune-mediated, logical factors, toxic, neurological and traumatic microcirculatory problems [1]. Cochlear or Inner Ear Hemorrhage (IEH) has been reported is a rare cause of sudden deafness, isolated cases are often described [3,4].
Case presentation
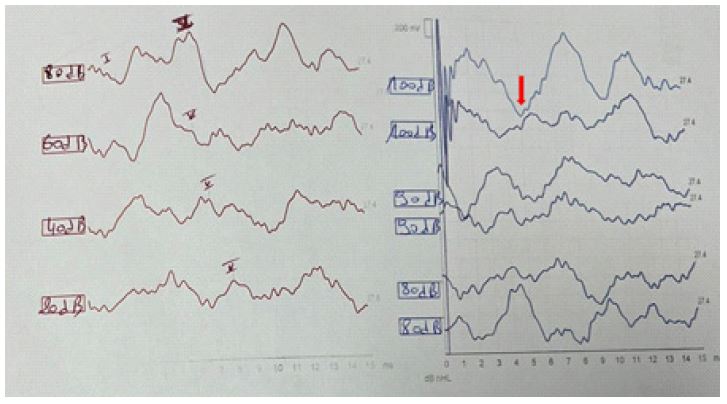
A 70-year-old man with a past history of diabetes mellitus and hypertension presented to our department with sudden onset hearing loss in his left ear over the thirty seven days. This was preceded by vertigo of the rotatory type a week earlier, which evolved into short, frequent attacks and permanent left-sided tinnitus. The patient denied any history of acoustic or traumatic trauma, medication use, or recent ENT infection. He denied Alcohol and tobacco consumption. Otoscopy was normal. Videonystagmoscopy showed spontaneous right horizontal nystagmus and no neurological deficit was found. There were no abnormalities in the laboratory tests. We found no infectious or inflammatory syndrome (white blood cell count 9800E/mm3 and CRP 8 mg/l). Sample and Covid-19 serology were negative. Tonal audiometry revealed a left unilateral subcochlear hearing loss with a hearing threshold of 100 dB, confirmed by auditory Brainstem Evoked Potentials (BER) (Figure 1).
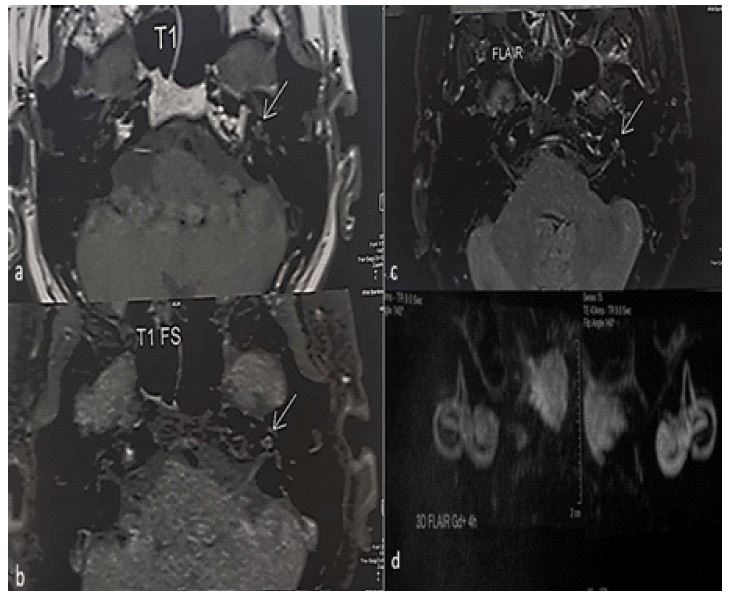
In view of the unilateral sensorineural hearing loss, an additional MRI of the inner ear was performed, including a 3D FLAIR sequence, which showed hight signal intensity in the left cochlea (Figure 2). The patient was diagnosed with a labyrinthine haemorrhage. On the basis of the imaging data, we completed the aetiological investigation, in particular with a haemostasis laboratory test, a nuclear antibody and tumour marker assay. The diagnosis of idiopathic cochlear haemorrhage was the most probable in view of the normality of tets and the absence of risk factors, in particular cervicofacial and cerebral radiotherapy, the use of antiplatelet or anticoagulant agents, or a history of meningitis.
The patient received intravenous corticoid therapy at a dose of 1 mg/Kg/day for 10 days, followed by oral doses with a gradual tapering. Additionally, the patient was administered vasodilators and underwent 15 sessions of hyperbaric oxygen therapy (2ATA per session, five sessions per week).
Since the seventh day of intravenous tretment and third oxygen therapy, the patient noted that the vertigo and the tinnitus disappeared. The improvement in hearing was partial, with a hearing threshold at the end of treatment of 75 dB. A hearing aid was prescribed. The patient reported a marked improvement in their condition and expressed hope to resume normal activities after the fitting.
Discussion
The diagnosis of haemorrhagia requires a combination of clinical and imaging data. Clinical data should include severe to profound deafness with a described hearing loss exceeding 80 dB and vertigo [4].
MRI allows diagnosis in the form of a spontaneous hypersignal T1, not enhanced by gadolinium injection due to the presence of methemoglobin appearing 48 hours after the hemorrhagic event. The sequence T2 signal varies according to the age of the hemorrhagic event (hyposignal initially, progressing to isosignal and then hypersignal) [3]. The radiological evolution is variable: persistence of the hypersignal, regression of the images and normalization or evolution towards sclerosing and ossifying labyrinthitis [5].
The pathophysiological characteristics are currently unclear but various etiologies for Inner Ear Hemorrhage (IEH) have been identified. Vascular aetiologias due to anticoagulant or antiaggregant seems the most implicated in cases of overdose [6]. In our study, our patient had not received any treatment that could have an effect on coagulation.
The second most common described etiology in the literature is hematological diseases such as myeloma, Waldenstrom’s disease, and autoimmune diseases such as rheumatoid arthritis and systemic lupus erythematosus or leukaemia [4]. Cell blood count, antinuclear antibodies and rheumatoid factor were negative in our case.
Meningitis with bacterial diffusion may also be involved, but the clinical presentation is different, with neurological symptoms [7]. Less frequently reported are the radiotherapy to the head and neck with cases reported twenty years after irradiation [8] and chemical attacks on the inner ear or toxic substances like cocaine causing IEH by vascular effects [9]. However, the cause cannot be determined, and many cases are considered idiopathic IEH. This was the case of our patient.
Management of IEH is not specific and patients are under corticoid associated to the etiological treatment. However, prognosis remain poor in reason of severe cochlea-vestibular lesion in comparison to other aetiologias of SSNHL. Many authors noted no significant improvement in early or late control [4,7,10]. Wu X et al. [10], in a comparative study of 30 patients with IEH vs 62 patients with no-hemorrhagic inner ear note that the second group have a better hearing recovery in the two weeks three and six months follow up (p< 0.05). A cochlear implantation was necessary for the case reported by Meunier and al. [4] in reason of bilateral profound hearing loss with bilateral IEH. In our case, patient have a partial improvement with 25 dB hearing gain with Tinnitus and vertigo disappears. In our knowledge, no other author has introduced hyperbaric oxygen therapy in the management of idiopathic or secondary IEH.
Conclusion
Inner ear hemorrhage is a rare cause of Sudden Sensorineural Hearing Loss (SSNHL). The diagnosis of IEH is based on clinical and imaging data. Before diagnosing idiopathic IEH, it is important to investigate the cause of the hemorrhage. Hower the prognosis for hearing loss in IEH cases is uncertain.
Informed consent: We have obtained an informed and signed consent of our patient for his case to be anonymously published.
Competing interests statement: The authors declare no competing interests.
References
- Shinohara S, Yamamoto E, Saiwai S, Tsuji J, Muneta Y, Tanabe M, et al. Clinical features of sudden hearing loss associated with a high signal in the labyrinth on unenhanced T1-weighted magnetic resonance imaging. Eur Arch Otorhinolaryngol. 2000; 257(9): 480-484.
- Stachler R.J, Chandrasekhar S.S, Archer S.M, et al. Clinical practice guideline: sudden hearing loss. Otolaryngology and Head and Neck Surgery. 2012; 146(3): 1-35.
- Jrad M, Zlitni H, Boumediene M, Nasr AB, Bouzrara M. Intracochlear Hemorrhage: A Rare Cause of Sudden Sensorineural Hearing Loss. Case Rep Radiol. 2021; 22: 1072047.
- Meunier A, Clavel P, Aubry K, Lerat J. A sudden bilateral hearing loss caused by inner ear hemorrhage. European Annals of Otorhinolaryngology, Head and Neck Diseases. 2020; 137(1): 56-67. (Article in french).
- Weissman JL, Curtin HD, Hirsch BE, Hirsch WL Jr. High signal from the otic labyrinth on unenhanced magnetic resonance imaging. AJNR Am J Neuroradiol. 1992; 13(4): 1183-1187.
- Arellano B, Brea B, González FM. Labyrinthine haemorrhage secondary to oral anticoagulants. Acta Otorrinolaringol Esp. 2016; 67(3): 185-186.
- Tan JH, Yeh BI, Seet CS. Deafness due to haemorrhagic labyrinthitis and a review of relapses in Streptococcus suis meningitis. Singapore Med J. 2010; 51(2): 30-33.
- Poh ACC, Tan TY. Sudden deafness due to intralabyrinthine haemorrhage: a possible rare late complication of head and neck irradiation. Ann Acad Med Singapore. 2007; 36(1): 78-82
- Nicoucar K, Sakbani K, Vukanovic S, Guyot J. P. Intralabyrinthine haemorrhage following cocaine consumption. Acta Otorrinolaringológica Española. 2005; 125(8): 899-901.
- Wu X, Liu M, Zhuang HW, Chen KT, Yang ZY, Xiong GX. Cochleo-vestibular lesions and prognosis in patients with profound sudden sensorineural hearing loss: a comparative analysis. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2020; 55(5): 472-478. (article in Chinese).