
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Neurocutaneous melanocytosis: A case report with antenatal presentation
Robinson R; Lloyd Tooke*
Department of Pediatrics, Groote Schuur Hospital, University of Cape Town, Cape Town, South Africa.
*Corresponding Author : Lloyd Tooke
Department of Pediatrics, Groote Schuur Hospital, University of Cape Town, Cape Town, South Africa.
Email: lloyd.tooke@uct.ac.za
Received : May 28, 2024
Accepted : Jun 06, 2024
Published : Jun 13, 2024
Archived : www.jcimcr.org
Copyright : © Tooke L (2024).
Abstract
Neurocutaneous melanocytosis is one of the neurocutaneous syndromes. This condition is a rare but serious congenital condition that is characterised by hyperpigmented melanocytic naevi of varying size and number with associated melanocytosis of the leptomeninges. This is a case of a newborn baby that was antenatally discovered to have dilated ventricles and on delivery found to have multiple hyperpigmented lesions over the skin suggestive of this condition. The clinical presentation, imaging and management of this condition is further discussed.
Keywords: Neurocutaneous syndrome; Neurocutaneous melanocytosis; Ventriculomegaly; Hyperpigmented lesions; Cranial ultrasound; MRI; Newborn.
Abbreviations: CT: Computed Tomography Scan; MRI: Magnetic Resonance Imaging; PET: Positron Emission Tomography.
Citation: Robinson R, Tooke L. Neurocutaneous melanocytosis: A case report with antenatal presentation. J Clin Images Med Case Rep. 2024; 5(6): 3119.
Introduction
Neurocutaneous melanocytosis (NCM) (MIM # 249400; ORPHA: 2481) is a congenital condition that is characterised by cutaneous hyperpigmented melanocytic naevi and excessive melanocyte proliferation of the leptomeninges. NCM (also sometimes known as neurocutaneous melanosis) falls into the larger group of neurocutaneous syndromes which affect structures primarily derived from the ectoderm such as the central nervous system, skin, and eyes. First described in 1861, NCM is rare (300 cases have been reported worldwide) [1], but it is beneficial to suspect and diagnose it early in life to anticipate and manage complications timeously.
There is no familial inheritance pattern and an equal incidence between males and females although there may be a higher propensity for complications in boys [2]. The exact cause is not clear however a mutation in the NRAS gene has been strongly associated with this condition [3].
Case study
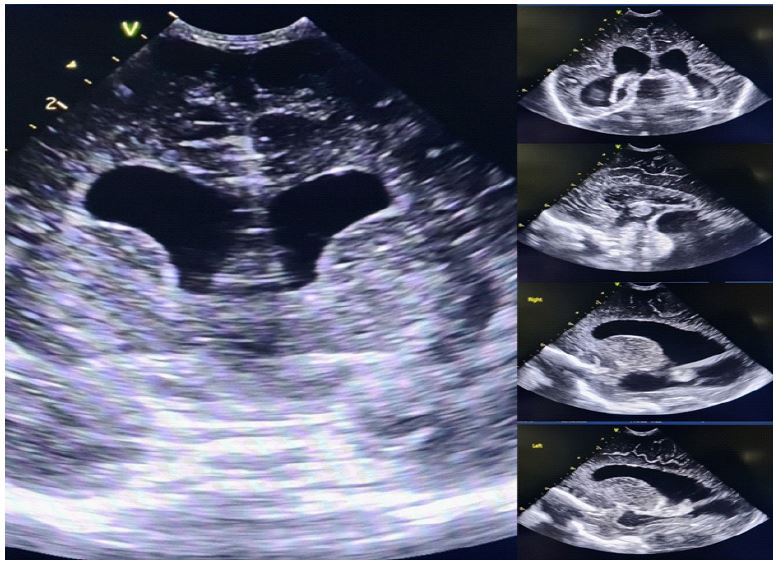
A female infant was born to a 27-year-old mother at term gestational age in Cape Town, South Africa [4]. Antenatal scans had been normal up until 20 weeks gestation, but at 35 weeks gestation, another scan identified bilateral cerebral ventriculomegaly. There was also a large dilated posterior fossa. This finding prompted delivery at the tertiary referral hospital. The infant was well at birth with a normal birthweight of 3370g. The clinical exam after delivery revealed no dysmorphic/syndromic features except for 14 melanocytic naevi of varying sizes distributed on the face, scalp, limbs and back, including a large hairy naevus over the left thigh (Figure 1). The head was normal shape but had an enlarged, but not bulging, anterior fontanelle with a head circumference of 37.5cm which was just above the 90th centile for gestational age. Neurological examination showed normal tone, movement, and primitive reflexes. The remainder of the physical exam was unremarkable. A cranial ultrasound was performed (Figure 2) which showed hypoplastic midline structures with a normal corpus collosum, massively dilated ventricles and a large cisterna magna. The cerebellum was difficult to appreciate due to the large cisterna magna however the vermis was thought to be present. The infant remained with the mother in the postnatal ward and by day 5 of life breast feeding had been well established. Due to the cutaneous and neurological findings, the genetic department thought NCM was the likely diagnosis. The neurosurgery team advised careful monitoring of the head circumference and the infant was to be followed weekly at the paediatric clinic at their local hospital in another town. Further appointments were made at neurology and dermatology clinics at the tertiary children’s hospital in Cape Town.
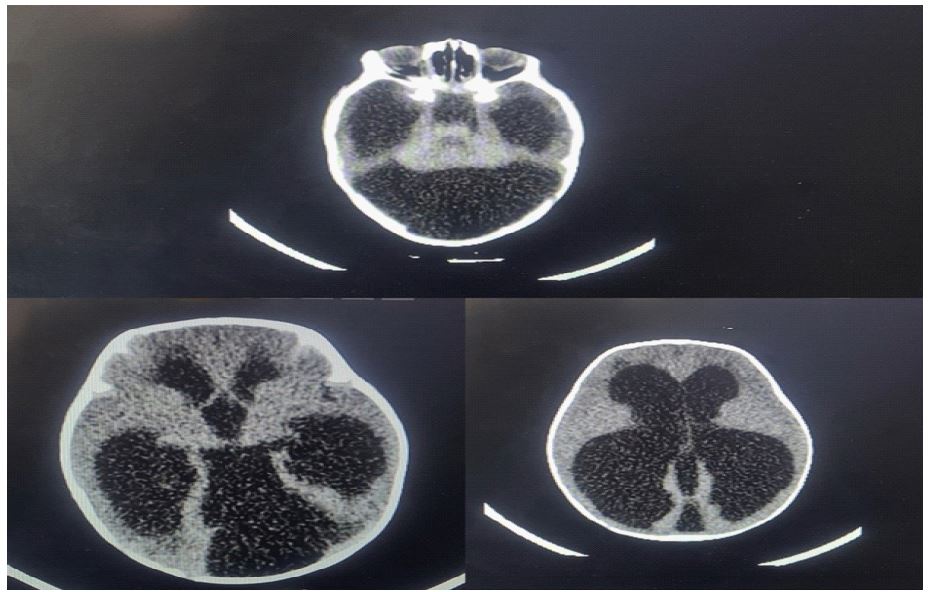
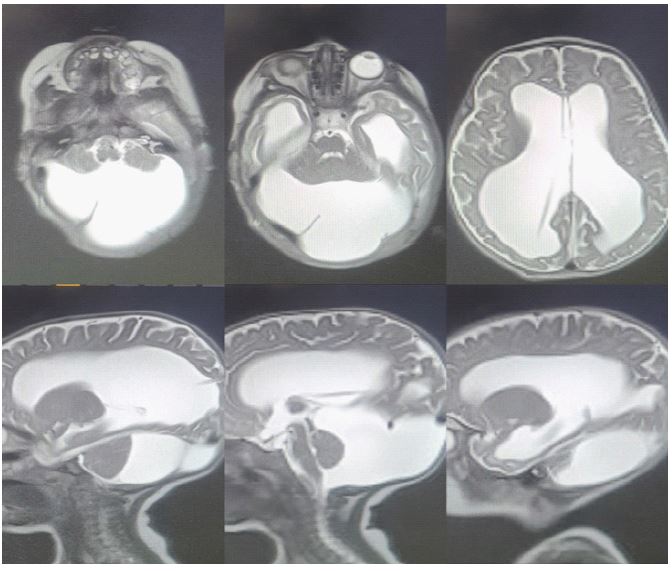
By 3 months of age the infant was admitted to the neurosurgical ward at Red Cross Children’s Hospital due to rapidly increasing head circumference. On admission the head circumference was 47cm (greater than the +3 WHO z-score). A CT brain revealed hydrocephalus with Dandy-Walker malformation complex (Figure 3). A right occipital ventriculoperitoneal (VP) shunt was inserted and a T2-weighted MRI confirmed correct placement of the shunt and better defined the posterior fossa. The MRI identified a large retro-cerebellar cyst with elevation of the tentorium cerebelli causing a mass effect on a small cerebellum. There was a large posterior fossa with the fourth ventricle communicating with the cyst. There was also compression of the cerebral cortices with no clear grey-white matter interface (Figure 4). No T1-weighted imaging was performed due to time constraints. Clinically the baby remained well, the lumbar puncture was clear, and she completed 24hrs of prophylactic antibiotics. The infant was discharged a few days later and follow up appointments at the local hospital and referral hospitals were planned.

Discussion
This infant was born with 14 congenital melanocytic naevi with one large lesion on the left thigh. Although rare, NCM should be considered when an infant is born with large and/or multiple (CMN). There is an increased risk of NCM if there are any large congenital melanocytic naevi. Approximately 12% of individuals with large CMN will develop NCM and conversely, of the patients with NCM, two thirds of them have at least one large lesion [1] Large naevi are often hairy and in neonates measure ≥6cm on the body or ≥9cm on the head. Although some researchers advocate the use of the term ‘giant’ for very large lesions [3], this has not widely been adopted and ‘large’ and ‘giant’ are often used interchangeably [5]. The number of smaller satellite lesions (typically more than 20) is also correlated with an increased risk of NCM.
Congenital melanocytic naevi of the skin and leptomeningeal/nervous system infiltration are usually benign but may rarely progress to melanoma or non-malignant melanosis of the brain [6]. The incidence of transformation of the naevi to melanoma is unknown however is thought to be in the range of 10 – 15% which can occur in the first decade of life [2].
Neurological: The infant in this report already had neurological complications which were picked up antenatally. On clinical exam, macrocephaly was present at birth. The nervous system manifestations of neurocutaneous melanocytosis usually appear within the first three years of life although an uncommon spike in occurrence occurs in the 2nd and 3rd decades of life occurs, and a solitary case of a patient exhibiting symptoms at age 65 has been described [3].
Neurological signs and symptoms are related to the presence of melanocytic lesions in the leptomeninges of the central nervous system. Mechanisms that lead to the manifestations of the disease in the nervous system include raised intracranial pressure, seizures, and spinal involvement.
The infant in this report had both hydrocephalus (which was progressive) and the Dandy-Walker malformation complex [3]. Hydrocephalus may occur due to the deposits of melanocytic cells in the leptomeninges which can prevent the reabsorption of CSF (communicating hydrocephalus) or due to aqueduct stenosis (non-communicating). The raised intracranial pressure caused by this may result in macrocephaly and enlarged fontanelles in infancy. Dandy-Walker malformation complex, is frequently associated with neurocutaneous melanocytosis, and is proposed to be a marker of profound infiltration of melanocytes in the nervous system [2,7].
Although no seizures had yet been noted in this infant [1], the manifestation of seizures is usually a sign of parenchymal involvement and can present in a variety of seizure forms e.g. generalised tonic-clonic, myoclonic or focal seizures. Infantile spasms, West syndrome and Lennox-Gastaut syndrome have also been described.
Associated intellectual disability and delayed milestones are variable and many are typically developing [1]. Spinal involvement is reported in patients that develop myelopathy, radiculopathy or bowel and bladder dysfunction. Other neurological syndromes such as spinal cord compression, secondary syringomyelia, arachnoiditis diffuse leptomeningeal thickening can occur [8].
Radiological findings: The infant in this report had features of hydrocephalus even during antenatal life. CT scanning and subsequent MRI allowed greater clarification of the extent of the hydrocephalous and brain structures. As the CT and MRI were performed peri-operatively for the ventriculoperitoneal shunt, their main purpose was to assist with the planning of the surgery and to confirm adequate placement of the shunt. The identification of melanocytic deposits was not the primary focus of the imaging.
Even though ultrasound scan is not diagnostic, along with accurate clinical history, radiological features such as echogenic lesions can be identified. However [9], the differential diagnosis for this may include haemorrhage, primary or metastatic neoplasm, and hamartomas in tuberous sclerosis. CT scan of a patient with NCM may reveal hypoplasia of the pons and cerebellum, however, the foci of the melanocytic lesions may only show subtle hypodensities. The modality of choice for the recognition of neurocutaneous melanocytosis is an MRI scan [2], preferably in the first few months of life. This is important because as the patient ages through the middle and later months of their first year of life, the brain becomes more and more myelinated, and it becomes more difficult to identify the melanocytosis. The typical finding for neurocutaneous melanocytosis is T1 shortening of the involved structures due to the presence of melanin pigment [2]. Hyperintensities along the leptomeninges and in the parenchyma are signs of melanocytic deposits and these show as hypointensities on T2 weighted imaging [3]. Other associated findings on MRI include Chiari 1 malformation, lissencephaly and Dandy-Waler malformation [10]. Spinal MRI may show spinal arachnoid cysts which are typically asymptomatic [10]. PET scans aren’t routinely done however can be used in patient follow up and may assist in detecting malignant transformation [1].
Management and prognosis: The number and prognosis of patients with asymptomatic NCM remains difficult to predict. However, if symptomatic, NCM remains a disease with a poor outcome. With the occurrence of neurological signs, the prognosis of the patient becomes poor as the progression of the disease leads to high mortality often within a few years of presentation [2]. Those infants such as this little girl who prespresent very early and those with Dandy-Walker malformation have the worst outcomes [3]. Interventions such as VP shunting are mainly palliative measures and chemotherapy for melanocytic proliferation or malignant change is currently ineffective [2].
The management of a patient with NCM requires input from a multi-disciplinary team including dermatology, plastic surgery, and neurology for the asymptomatic patient, and added input from radiology, neurosurgery and possibly oncology in the symptomatic patient. Early imaging allows the distinguishing of melanocytosis in the brain.
Ongoing psychological support is important for the wholistic management of the patient and family and even more so when the prognosis is extremely poor.
Conclusion
Neurocutaneous melanocytosis is a rare but serious condition which can present in the antenatal period. It should be considered when infants are born with large and/or multiple CMN. Although outcomes remain poor in symptomatic patients, it is important to manage complications with a multidisciplinary team and support the families wholistically.
Disclosure: The authors declare that they have no conflicts of interest concerning this article.
References
- Flores-Sarnat L. Neurocutaneous melanocytosis. Handbook of clinical neurology. 2013; 111: 369-88.
- Ruggieri M, Polizzi A, Catanzaro S, Bianco ML, Praticò AD, Di Rocco C. Neurocutaneous melanocytosis (melanosis). Child’s Nervous System. 2020; 36: 2571-96.
- Scattolin M, Lin J, Peruchi M, Rocha A, Masruha M, Vilanova L. Neurocutaneous melanosis: follow-up and literature review. Journal of Neuroradiology. 2011; 38(5): 313-8.
- Charbel C, Fontaine RH, Malouf GG, Picard A, Kadlub N, El-Murr N, et al. NRAS mutation is the sole recurrent somatic mutation in large congenital melanocytic nevi. Journal of Investigative Dermatology. 2014; 134(4): 1067-74.
- Ruiz‐Maldonado R. Measuring congenital melanocytic nevi. Pediatric dermatology. 2004; 21(2): 178-9.
- Marghoob AA, Dusza S, Oliveria S, Halpern AC. Number of satellite nevi as a correlate for neurocutaneous melanocytosis in patients with large congenital melanocytic nevi. Archives of dermatology. 2004; 140(2): 171-5.
- Marnet D, Vinchon M, Mostofi K, Catteau B, Kerdraon O, Dhellemmes P. Neurocutaneous melanosis and the Dandy–Walker complex: an uncommon but not so insignificant association. Child’s Nervous System. 2009; 25: 1533-9.
- Ramaswamy V, Delaney H, Haque S, Marghoob A, Khakoo Y. Spectrum of central nervous system abnormalities in neurocutaneous melanocytosis. Developmental Medicine & Child Neurology. 2012; 54(6): 563-8.
- Chen YA, Woodley-Cook J, Sgro M, Bharatha A. Sonographic and magnetic resonance imaging findings of neurocutaneous melanosis. Radiology Case Reports. 2016; 11(1): 29-32.
- Islam MP. Neurocutaneous melanosis. Handbook of Clinical Neurology. 2015; 132: 111-7.