
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
An unusual diagnosis of superior oblique palsy: A case of congenital absence of bilateral superior oblique muscle?
Yongguang Yuan; Chonglin Chen; Ruixin Wang; Jianhua Yan; Xinping Yu*
State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangzhou, China.
*Corresponding Author : Xinping Yu
State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangzhou, China.
Email: yuxinping@gzzoc.com
Received : May 21, 2024
Accepted : Jun 07, 2024
Published : Jun 14, 2024
Archived : www.jcimcr.org
Copyright : © Yu X (2024).
Abstract
Imaging of Superior Oblique Palsy (SOP) consistently shown a variable degree of hypoplasia of the paretic Superior Oblique muscle (SO) and variable trochlear nerve absence. But SO absence is very rare in imaging examination, especially in both eyes.
Keywords: Superior oblique palsy; Superior oblique muscle absence; Strabismus surgery.
Citation: Yuan Y, Chen C, Wang R, Yan J, Yu X. An unusual diagnosis of superior oblique palsy: A case of congenital absence of bilateral superior oblique muscle. J Clin Images Med Case Rep. 2024; 5(6): 3121.
Introduction
Superior Oblique Palsy (SOP) is the most common type of vertical deviation, characterized by hypertropia of the paretic eye and hypertropia worsening in addution of paretic eye and Abnormal Head Posture (AHP). However, bilateral SOP show a remarkable V pattern and excyclotropia of fundus. The main clinical treatment methods include prism, botulinum toxin injection of ipsilateral inferior oblique muscle and surgery management.
Case presentation
A 7-year-old female presented with outward and upward deviations in either her right or left eye. When looking to the right, the deviation of her left eye was notably more pronounced. Conversely, when gazing to the left, her right eye also exhibited hyper-deviation without AHP.
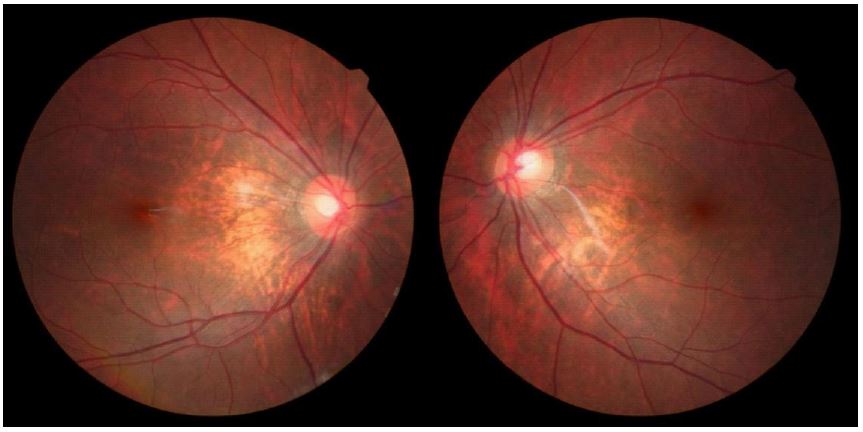
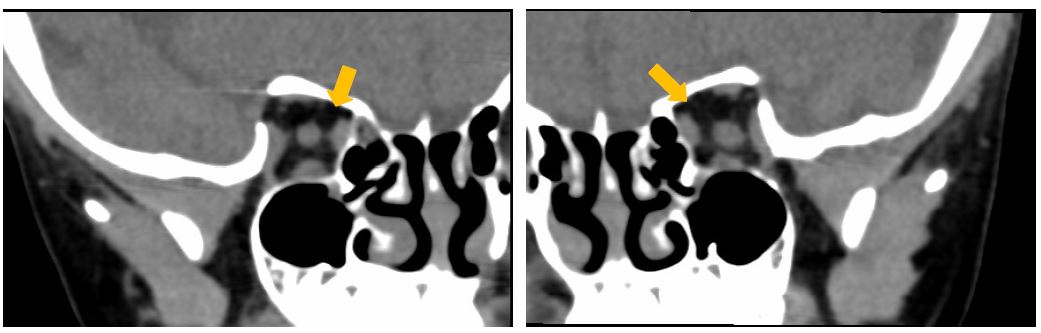
The nine-gaze photograph revealed profound underaction of the SO in both eyes, measuring at -4, coupled with pronounced overaction of the Inferior Oblique muscles (IO), graded at +3 (Figure 1). In primary position, the exodeviation measured 40 PD at distance and 45 PD at near when either the right or left eye served as the fixating eye. When looking upwards, the exodeviation intensified to 45 PD, while downward gaze resulted in a decrease to 20 PD, indicative of a V-pattern exotropia. Fundus photos show a remarkable excyclotropia in left eye (Figure 2). Orbital CT examination: CT scans disclosed a virtually absence of bilateral SO in both axial and coronal sections, as indicated by the orange arrows in Figure 3. Therefore, clinical diagnosis is congenital SOP (OU) and V pattern exotropia (OU). To treat V pattern exotropia, Bilateral Lateral Rectus Recession (BLR) and inferior oblique muscle anterior transposition (IOAT).
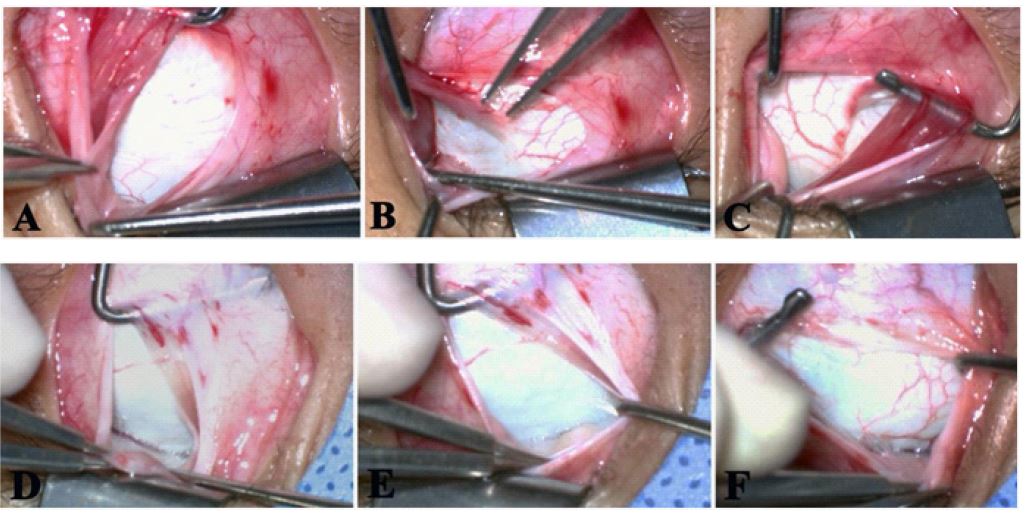
In accordance with the findings from the orbital CT, an exploratory examination of the SO was carried out across its temporal aspect (depicted in Figure 4A,D), inferior aspect (Figure 4 B,E), and nasal aspect of the superior rectus muscle (Figure 4C, F), denoted by the orange arrow. This exploration revealed the absence of any SO tendon in either eye. Therefore, this is a case of congenital bilateral SO absence.
Discussion
The congenital absence of SO is a highly unusual phenomenon, yet it stands as the most prevalent among all congenital absence of EOMs [1-8]. Notably, many patients initially identified as having an absent SO tendon during strabismus surgery are, in fact, suffering from agenesis of SO. Some cases involve the absence of a SO tendon, yet coronal or axial MRI scans can still reveal attenuated remnants of the SO bellies [2]. Whether occurring unilaterally or bilaterally, the absence of SO invariably manifests as Superior Oblique Palsy (SOP), a predominant form of incomitant vertical strabismus. SOP is typified by hypertropia of the affected eye, SOUA and IOOA (or either of these conditions), along with compensatory head tilts and a positive Bielschowsky test. Other characteristic clinical presentations include V-pattern strabismus, excyclotorsion, atrophy or absence of SO as discerned from orbital imaging studies. Bilateral SOP typically presents with more pronounced excyclotorsion, a more exaggerated V-pattern deviation, alternating hypertropia in right or left gaze (with right hypertropia when gazing left and left hypertropia when gazing right), and a positive Bielschowsky test in both eyes.
While congenital absence of SO is indeed infrequent, accurate preoperative diagnosis is crucial given the various surgical strategies involved. The following factors, often indicative of severe SOP, can also suggest congenital absence of SO [1,3-6]. (1) A conspicuously large and persistent vertical deviation in primary gaze, (2) Severe SOUA, as evidenced by a grade of -4 deficiency, (3) Absence of Abnormal Head Position (AHP), (4) Coexisting V-pattern horizontal deviation, (5) Most significantly, confirmation of SO absence in both coronal and axial sections via CT/MRI scans of the orbit, (6) Lastly, the inability to visually identify or palpate the SO tendon during surgical exploration. It is worth noting, however, that when the SO tendon is not encountered during surgery, it may not necessarily imply complete absence; the muscle could possess an exceptionally abnormal insertion or be profoundly hypoplastic. The absence of SO is relatively more prevalent in patients with craniofacial dysostoses, such as Crouzon’s syndrome and similar conditions.
Orbital imaging using MRI/CT scans plays a pivotal role in the assessment of congenital SOP. Consistent with prior research involving MRI analysis of SOP cases, there is frequently a variable extent of hypoplasia of the affected SO, with the muscle volume in the paretic eye commonly appearing significantly smaller compared to the unaffected eye [7]. Observations have indicated that the degree of muscle hypoplasia in congenital SOP cases can vary widely, spanning a continuum from complete aplasia to nearly normal development. In a study focusing on individuals with congenital SOP, 73% of subjects presented with an absent ipsilateral trochlear nerve and varying degrees of SO hypoplasia, whereas 27% had a seemingly normal SO and trochlear nerve bilaterally [7]. Sato et al. noted that in congenital SOP, there are two predominant peaks in the distribution of muscle size as a percentage of the normal side: one between 20% and 40%, and another between 90% and 100% [2]. Consequently, a broad spectrum of SO hypoplasia is typical among patients with congenital SOP, but a complete absence of SO is extremely uncommon [8]. Our patient exhibits a total absence of bilateral SO, representing an extremely rare condition.The ratio of the paretic to normal side SO volume offers exceptional predictive value in diagnosing congenital SOP. Thus, we recommend that orbital imaging should be considered a standard component of the diagnostic workup for SOP.
Clinically distinguishing the presence or absence of the trochlear nerve in patients with congenital SOP poses a challenge, necessitating the use of high-resolution MRI technology, ideally with a 3 Tesla (3T) system or above, utilizing 0.25 mm section thickness and an oblique axial scanning plane aligned parallel to the trajectory of the trochlear nerve, combined with expert interpretation [5]. Yang and colleagues have demonstrated that the ratio of paretic to normal side SO volume, as well as the area measurement at the optic nerve-globe junction, provides an excellent predictive indicator for trochlear nerve absence. They concluded that patients with congenital SOP exhibiting a substantial SO hypoplasia of ≤75% relative to the unaffected side are more likely to have an absent trochlear nerve [5]. In light of these findings, it is plausible that our patient may have bilateral absence of the trochlear nerve.
Conclusion
Orbital imaging using MRI/CT scans plays an important role in the assessment of congenital SO absence, but an exploratory examination can provide more evidence to support our diagnosis. In spite of this, IO weakening surgery can still effectively improve the coordination of eye movements.
References
- Mumma JV. Surgical procedure for congenital absence of the superior oblique. Arch Ophthalmol. 1974; 92(3): 221-223.
- Sato M. Magnetic resonance imaging and tendon anomaly associated with congenital superior oblique palsy. Am J Ophthalmol. 1999; 127: 379-387.
- Wallace DK, von Noorden GK. Clinical characteristics and surgical management of congenital absence of the superior oblique tendon. Am J Ophthalmol. 1994; 118(1): 63-69.
- Chan TK, Demer JL. Clinical features of congenital absence of the superior oblique muscle as demonstrated by orbital imaging. J AAPOS. 1999; 3(3): 143-150.
- Yang HK, Lee DS, Kim JH, Hwang JM. Association of superior oblique muscle volumes with the presence or absence of the trochlear nerve on high-resolution MR imaging in congenital superior oblique palsy. AJNR Am J Neuroradiol. 2015; 36(4): 774-778.
- Matsuo T, Ohtsuki H, Sogabe Y, Konishi H, Takenawa K, et al. Vertical abnormal retinal correspondence in three patients with congenital absence of the superior oblique muscle. Am J Ophthalmol. 1988; 106(3): 341-345.
- Yang HK, Kim JH, Hwang JM. Congenital superior oblique palsy and trochlear nerve absence: a clinical and radiological study. Ophthalmology 2012; 119: 170-177.
- Gore DM, Malik NN. Fourth nerve palsy associated with almost complete absence of the superior oblique muscle. Can J Ophthalmol. 2006; 41(6): 784-785.