
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Complete heart block; a clue to Kearns-Sayre syndrome: A case report
Tarek Hammouda1,2*; Wessam Ali1; Mohamed Sayed1; Aliaa Tarek1; Ahmed Nasr1; Dina Haroun1; Omnia Kamel1
1Aswan Heart Center, Magdi Yacoub Foundation, Egypt.
2Department of Cardiology, Kasr Al Ainy, Cairo University Hospitals, Egypt.
*Corresponding Author : Tarek Hammouda
Aswan Heart Center, Magdi Yacoub Foundation, Egypt.
Email: tarek7ammouda@hotmail.com
Received : May 20, 2024
Accepted : Jun 07, 2024
Published : Jun 14, 2024
Archived : www.jcimcr.org
Copyright : © Hammouda T (2024).
Abstract
Background: High-grade AV block affects around 0.04% of the population. In the elderly, it is mostly attributed to age-related conduction system degeneration. On the other hand, high-grade AV block in young adults is rare. It prompts the search for a structural abnormality or a systemic disease such as infections, auto-immune diseases, sarcoidosis, and rare diseases as mitochondrial mutation syndromes.
Case summary: We present a case of a 25-year-old female presented with complete AV block. The patient had generalized weakness, progressive diminution of vision over 15 years until she became blind due to pigmentary retinopathy, with increased fatiguability over the last year. Neurological examination revealed symmetrical upper and lower limb weakness, generalized muscle wasting, and hypotonia. This, together with evident ptosis in the examination, suggested a rare mitochondrial disorder known as Kearns-Sayer syndrome, which is a triad of ophthalmoplegia, pigmentary retinopathy, and early onset before 20 years of age, together with either heart block, cerebellar ataxia, or cerebrospinal fluid protein greater than 100 mg/dL. The patient was treated with the implantation of a permanent pacemaker. There are no other drugs or treatment modalities proven to improve the vision or myopathy in this disease.
Conclusion: Complete heart block in young people should prompt an extensive search for the etiology. Kearns-Sayre syndrome is a rare disease that can cause complete AV block, leading to sudden cardiac death. So, such patients should be followed closely by regular ECGs. Syncope or bifasicular block may provide an indication for early pacemaker implantation.
Keywords: Kearns-Sayre syndrome; Heart block in young; Pigmentary retinopathy; Mitochondrial mutation syndrome; Case report.
Citation: Hammouda T, Ali W, Sayed M, Tarek A, Nasr A, et al. Complete heart block; a clue to Kearns-Sayre syndrome: A case report. J Clin Images Med Case Rep. 2024; 5(6): 3122.
Introduction
High-grade AV block affects around 0.04% of the general population [1]. Its incidence increases with age and is higher in the presence of structural heart disease. On the other hand, high-grade AV block in young adults is rare, and if no cardiac structural abnormalities are found, it prompts the search for systemic diseases such as infections like Lyme’s disease, Chagas disease, auto-immune diseases, sarcoidosis, and rare diseases like mitochondrial mutation syndromes.
Kearns-Sayre syndrome is a rare mitochondrial syndrome caused mainly by large-scale mitochondrial DNA deletions or mitochondrial DNA depletion. The syndrome is defined by the obligatory triad of onset before the age of 20 years, progressive external ophthalmoplegia, and pigmentary retinopathy. In addition, at least one of the following must be present: heart block, cerebellar ataxia, or cerebrospinal fluid protein greater than 100 mg/dL. Cardiac manifestations in KSS are as high as 50%, and sudden cardiac death is reported in up to 23%. Sudden death is caused mainly by complete AV block or less commonly [2], ventricular arrhythmias [3].
Case timeline
| At age of 10 years | Progressive diminution of vision due to pigmentary retinopathy |
| At age of 20 years | Generalized weakness |
| At age of 24 years | Increased fatigability and occasional dizziness |
| At age of 25 years | Diagnosed to have complete AV block, received a VVI pacemakerClinical diagnosis of Kearns-Sayre syndrome |
Case details
The patient is a 25-year-old female. She started to complain of progressive diminution of vision 15 years ago and was diagnosed with pigmentary retinopathy, which ended in blindness. At the age of 20 years, she started to complain of a slowly progressive generalized weakness. Over the last year, she developed fatigue and occasional dizziness with no history of syncope. On a general check-up, the patient was diagnosed to have a complete AV block and was referred to our institute.
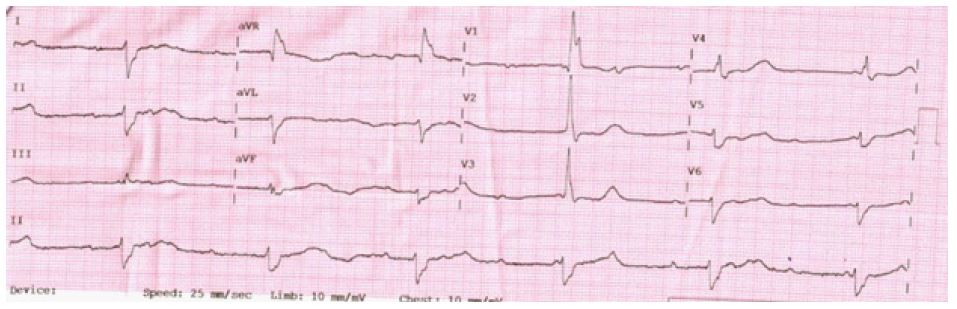
On assessment, the patient’s weight was 33 kg, and her height was 150 cm. She had ptosis. Neurological examination revealed symmetrical upper and lower limb weakness (limb motor power: grade 4/5), generalized muscle wasting, and hypotonia. Her ECG showed complete AV block with a wide escape rhythm (Figure 1). On doing echocardiography, normal LV internal dimensions and systolic function were detected. No evident valve abnormalities, no regional wall motion abnormalities, and no evidence of septal defects or infiltrative heart disease were found.
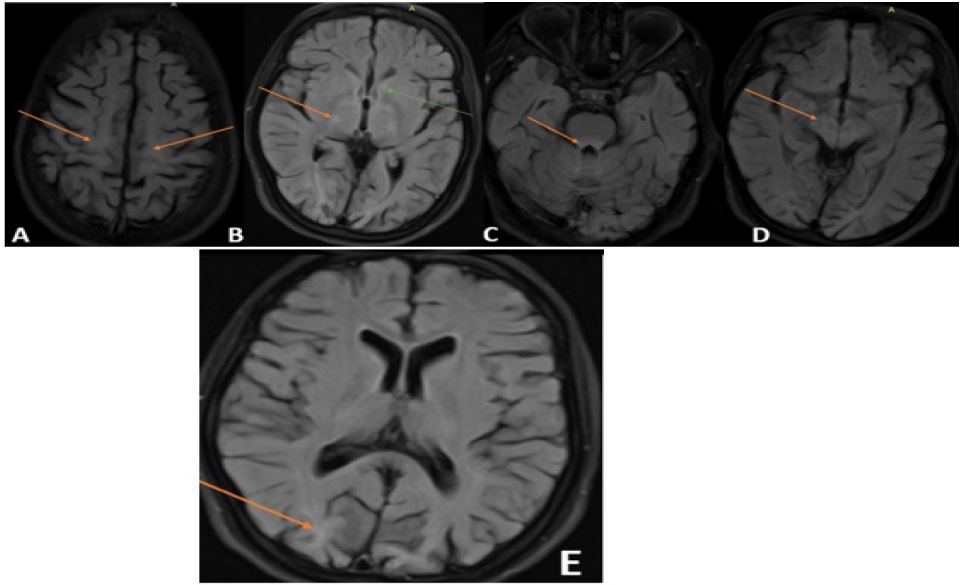
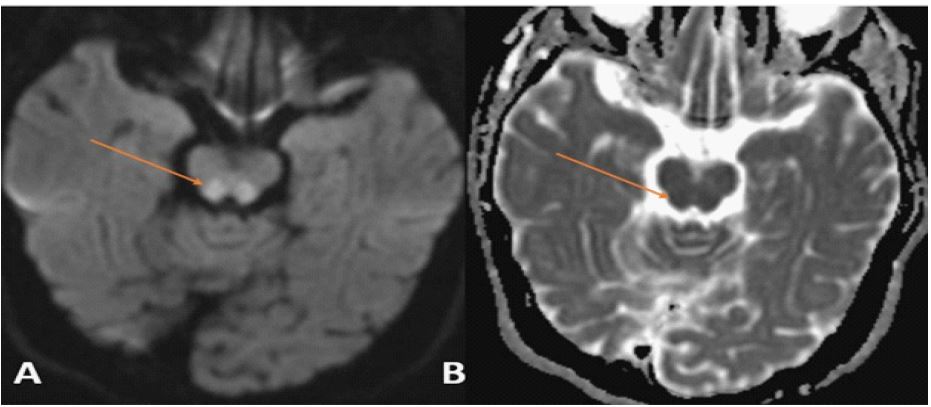
Brain MRI was performed and revealed high signal intensity at T2 and FLAIR involving subcortical white matter U fibers at the parietal areas, thalami, basal ganglia and brain stem. Cerebral atrophy was noted in the subcortical white matter at the occipital region. There was also bilateral focal symmetrical diffusion restriction on DW1 at the tectum of mid-brain (Figures 2 and 3).
Birth defects, myocardial ischemia, autoimmune conditions, Lyme disease complications, sarcoidosis, endocarditis, druginduced especially beta blockers and calcium channel blockers, post-valve surgeries, and rare syndromes such as mitochondrial DNA mutations causing Kearns-Sayre syndrome are all possibilities for high-grade AV block in young patients.
Based on the clinical manifestations, the patient was diagnosed as a case of Kearns-Sayre syndrome. We implanted a permanent pacemaker for her heart block. She was referred to a neurologist to follow up on her motor weakness.
Follow up and outcome: The patient had improvement of functional capacity. We noticed delayed wound healing.
Discussion
Kearns-Sayre syndrome is a mitochondrial encephalomyopathy characterized by deletions in mitochondrial DNA due to spontaneous mutations. Clinical presentation varies depending on the affected tissues. It usually manifests in children under 20 years with ataxia, ophthalmoplegia, retinitis pigmentosa, and cardiac conduction blockages. Infrequently, sensorineural hearing loss, dementia, muscle weakness, and endocrine abnormalities can occur. Although not always present at diagnosis, Conduction abnormalities of any degree are present in at least 50% of cases. In one case series of 35 cases, 34 patients developed a degree of conduction abnormality (heart block or conduction delays). The occurrence of high-grade AV block and, less frequently, ventricular arrhythmias (occasionally also bradycardia-related) is responsible for a high rate of sudden cardiac death; approximately 20% [4].
Diagnosis is made by the combination of clinical, radiologic, pathological anatomy, biochemistry, and molecular abnormalities [5].
Histopathologically, it is a disease characterized by spongiform degeneration (vacuolization) of nervous tissue, and its most frequent radiological findings in MRI are cerebral and cerebellar atrophy, with bilateral hyperintense lesions, in the peripheral subcortical white matter, U fibers, substantia nigra, globus pallidus, and brain stem (Subcortical white matter is usually abnormal). It is characteristic to observe diffusion restriction (hyperintensity of the signal in the diffusion enhanced sequence) of the affected white matter.
Currently, there is no definitive treatment for this disease [6]. High-grade AV blocks are managed by permanent pacemaker implantation. Due to the high risk of development of conduction disorders, regular ECG follow-up is warranted when an established diagnosis is made, with special emphasis on the PR interval and QRS width. The presence of bifasicular block may warrant an EP study to assess HV time and support the decision of prophylactic pacemaker implantation.
Ventricular arrhythmias are usually attributed to bradycardia. However, in one case report, a patient with a pacemaker died due to ventricular arrhythmia [4,7,9]. This supports the idea of implanting a dual chamber ICD whenever ventricular arrhythmias are detected [10].
Folinic acid supplementation for those with low CSF folate levels may alleviate fatigue and improve weakness.
Regarding genetic counseling, mitochondrial DNA deletion syndromes are caused by a single large-scale deletion in the mtDNA genome [11]. A mtDNA deletion may occur de novo or be transmitted through maternal (oocyte) inheritance. The father of a proband is not at risk of having the mtDNA pathogenic variant. The mother of a proband with a mtDNA deletion syndrome is usually unaffected and does not have mtDNA deletions in her somatic tissue; however, she may potentially harbor the mtDNA deletion in a population of her oocytes. If the mother of a proband is clinically unaffected, the risk to the sibs of a proband is estimated to be 1-4% because of the possibility of maternal germline mosaicism. Offspring of a female proband have up to a 4% risk of being affected. Offspring of a male proband with a mtDNA pathogenic variant are not at risk of inheriting the variant or manifesting the condition. Prenatal testing for pregnancies at increased risk is possible; however, prenatal test results cannot reliably predict phenotype [12].
Our case is a late presenter of this syndrome. She was only diagnosed to have kearns-Sayre syndrome after occurrence of the complete heart block which was the clue for her disease.
Learning points:
• Complete AV block in young should prompt extensive search for a cause.
• Kearns Sayre syndrome is a triad of ophthalmoplegia, pigmentary retinopathy, early onset before 20 years of age and either heart block, ataxia, or cerebrospinal fluid protein more than 100 mg/dL.
• Sudden death in Kearns-Sayre syndrome is caused by cardiac causes, complete AV block or ventricular arrhythmias.
• Kearns-Sayre syndrome patients should have regular ECG follow ups.
Declarations
Ethics apptoroval and consent participate: Signed consent on admission for use of case findings in research.
Consent for publication: Not needed. No personal data used.
Availability of data and material: All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Competing interests: Nothing to declare.
References
- Ostrander Jr LD, BRANDT RL, KJELSBERG MO, EPSTEIN FH. Electrocardiographic findings among the adult population of a total natural community, Tecumseh, Michigan. Circulation. 1965; 31(6): 888-98.
- Maceluch JA, Niedziela M. The clinical diagnosis and molecular genetics of kearns-sayre syndrome: a complex mitochondrial encephalomyopathy. Pediatr Endocrinol Rev. 2006; 4(2): 117-37.
- Kabunga P, Lau AK, Phan K, Puranik R, Liang C, Davis RL, Sue CM, Sy RW. Systematic review of cardiac electrical disease in Kearns–Sayre syndrome and mitochondrial cytopathy. International Journal of Cardiology. 2015; 181: 303-10.
- Khambatta S, Nguyen DL, Beckman TJ, Wittich CM. Kearns–Sayre syndrome: a case series of 35 adults and children. International journal of general medicine. 2014; 7: 325.
- Chawla S, Coku J, Forbes T, Kannan S. Kearns-Sayre syndrome presenting as complete heart block. Pediatric Cardiology. 2008; 29(3): 659-62.
- Moscatelli M, Ardissone A, Lamantea E, Zorzi G, Bruno C, Moroni I, Erbetta A, Chiapparini L. Kearns-Sayre syndrome: expanding spectrum of a “novel” mitochondrial leukomyeloencephalopathy. Neurological Sciences. 2022; 43(3): 2081-4.
- Beynum IV, Morava E, Taher M, Rodenburg RJ, Karteszi J, Toth K, Szabados E. Cardiac arrest in Kearns–Sayre syndrome. InJIMD Reports-Case and Research Reports, 2011/2. 2011; 7-10). Springer, Berlin, Heidelberg.
- Trivedi M, Goldstein A, Arora G. Prophylactic pacemaker placement at first signs of conduction disease in Kearns–Sayre syndrome. Cardiology in the Young. 2018; 28(12): 1487-8.
- Di Mambro C, Tamborrino PP, Silvetti MS, Yammine ML, Marcolin C, Righi D, Baban A, Martinelli D, Dionisi Vici C, Drago F. Progressive involvement of cardiac conduction system in paediatric patients with Kearns–Sayre syndrome: how to predict occurrence of complete heart block and sudden cardiac death?. EP Europace. 2021; 23(6): 948-57.
- Krishna MR. Kearns Sayre Syndrome: looking beyond AV conduction. Indian Pacing and Electrophysiology Journal. 2017; 17(3): 78-80.
- uijada-Fraile P, O’Callaghan M, Martín-Hernández E, Montero R, Garcia-Cazorla À, de Aragón AM, Muchart J, Málaga I, Pardo R, García-Gonzalez P, Jou C. Follow-up of folinic acid supplementation for patients with cerebral folate deficiency and Kearns-Sayre syndrome. Orphanet journal of rare diseases. 2014; 9(1): 1-9.
- Goldstein A, Falk MJ. Mitochondrial DNA Deletion Syndromes. In: GeneReviews®. University of Washington, Seattle, Seattle (WA). 1993. PMID: 20301382.