
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
Optical coherence tomography angiography features of retinal artery occlusion: A case series
Mojtaba Abrishami; Mehrdad Moatamed Shariati; Mohammad Reza Ansari Astaneh; Hamid Reza Heidarzadeh*
Eye Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
*Corresponding Author : Hamid Reza Heidarzadeh
Eye Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
Tel: + 98-51-37245363, Fax: +98-51-37285290;
Email: Dr.hamidreza.heidarzade@gmail.com
Received : May 26, 2024
Accepted : Jun 10, 2024
Published : Jun 17, 2024
Archived : www.jcimcr.org
Copyright : © Heidarzadeh HR (2024).
Abstract
Purpose: This study aims to assess the retinal vascular layers in Retinal Artery Occlusion (RAO) cases using Optical Coherence Tomographic Angiography (OCTA).
Methods: The study included three eyes of three patients with RAO. RAO was defined as sudden vision loss, retinal whitening, and inner retinal intracellular edema disrupting the retinal layers on the Optical Coherence Tomography (OCT) B-scan. OCTA cube scans were obtained using the RTVue-XR Avanti AngioVue. The images of the superficial and deep capillary plexuses were analyzed and compared with structural OCT.
Results: The OCTA findings revealed reduced vascular perfusion in both the superficial and deep capillary plexuses, corresponding to the areas of the inner retinal changes observed on OCT B-scan and fundus changes. Only large vessels were imaged, and no vascular flow was observed in the area nourished by the occluded microvascular bed. There was minimal alteration in the outer retina and choriocapillaris vascular flow.
Conclusion: OCTA is a valuable diagnostic tool for demonstrating the features necessary to diagnose RAO. Compared to FA, OCTA is fast, noninvasive, and provides improved visualization of microvascular details.
Keywords: Central Retinal Artery Occlusion (CRAO); Branch Retinal Artery Occlusion (BRAO); Optical Coherence Tomographic Angiography (OCTA); Optical coherence tomography.
Citation: Abrishami M, Shariati MM, Astaneh MRA, Heidarzadeh HR. Optical coherence tomography angiography features of retinal artery occlusion: A case series. J Clin Images Med Case Rep. 2024; 5(6): 3125.
Introduction
In the circulation of the retina, the blood flow in the inner retinal layers comes entirely from the Central Retinal Artery (CRA) unless a cilioretinal artery is present. The central retinal artery divides into four branches, each supplying one quadrant [1]. Histologic studies have shown that three levels of capillaries supply the inner retina: the radial peripapillary network in the Nerve Fiber Layer (NFL) in the peripapillary area, the Superficial Capillary Plexus (SCP), and the Deep Capillary Plexus (DCP) on either side of the Inner Nuclear Layer (INL). In Retinal Artery Occlusion (RAO) cases, disruption of the blood flow in the inner retina can lead to sudden visual loss due to ischemia, retinal edema, and thickening in the acute phase [2]. The severity of these effects depends on which groups of capillaries are involved [3]. Optical Coherence Tomography Angiography (OCTA) is a new non-invasive high-speed imaging technique that can evaluate retinal circulation within seconds. It is a novel technique that can show the blood flow in each layer separately without the need for dye injection, providing clinicians with the ability to analyze the microvascular structure of the retina. Few reports are available regarding the application of OCTA in evaluating retinal vascular layers in RAOs [4]. This study aims to evaluate these layers in RAOs imaged by OCTA.
Methods
Study population: This study is an observational case series of patients with Central and Branch Retinal Artery Occlusion (CRAO and BRAO) conducted at Khatam Eye Hospital, a tertiary referral ophthalmology center affiliated with Mashhad University of Medical Sciences. The patients experienced sudden visual loss, and clinical signs confirmed their diagnoses. Imaging of the superficial and deep capillary plexus was performed using OCTA.
Imaging procedure: The AngioVue instrument, based on Optovue RTVue XR Avanti technology, was used to capture OCTA images to obtain amplitude-decorrelation angiography images. Default preset parameters were used to segment the capillary bed. The SCP (superficial capillary plexus) became visible when the “en-face” image was segmented between an inner boundary at 3 μm beneath the ILM and an outer boundary at 15 μm beneath the Inner Plexiform Layer (IPL). The en-face image of the DCP (Deep Capillary Plexus) was obtained by setting the inner and outer boundaries at 15 μm and 70 μm beneath the IPL, creating a 55 μm thick slab. Best-Corrected Visual Acuity (BCVA) measurements were also taken.
Ethical issues: The Ethical Committee of the Research Deputy of Khatam Eye Hospital (Mashhad University of Medical Sciences, Mashhad, Iran) approved the study and its data acquisitions. Patients were enrolled in the study after providing written informed consent in compliance with the Declaration of Helsinki.
Results
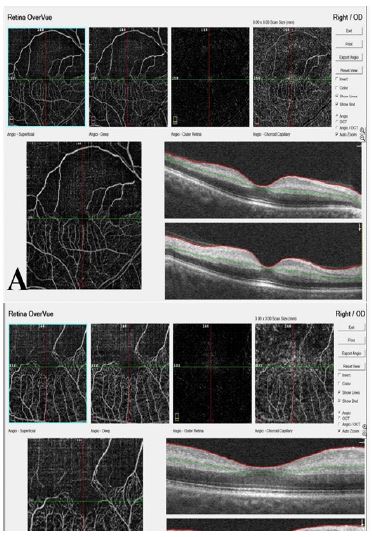
Case 1: A 70-year-old male presented with a sudden, painless loss of vision in his right eye for two days. He has had hypertension for fifteen years. His vision in the right eye was poor (1-meter finger counting), while his left eye was 20/32. A Relative Afferent Pupillary Defect (RAPD) was positive in the right eye. The anterior segment examination was normal for both eyes, except for a non-significant cataract. The Intraocular Pressure (IOP) was 12 mmHg for the right eye and 13 mmHg for the left eye. Fundus examination revealed edematous and white retinae around the superior arcade of the right eye. The diagnosis was confirmed as Branch Retinal Artery Occlusion (BRAO) based on retinal edema in the superior hemifield and retinal intracellular edema in the OCT images. OCTA showed decreased flow in the superior arcade and remarkably decreased perfusion in the upper half of the image’s superficial and deep capillary plexus. The Foveal Avascular Zone (FAZ) became half disrupted, with only an inferior semicircle remaining from the normal circular FAZ boundary. In the superior hemifield, except for flow in the large vessels, no other flow was documented in the 3×3 or 8×8 mm OCTA images.
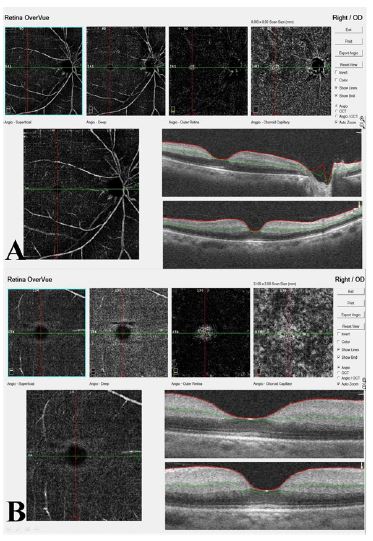
Case 2: A 65-year-old man with a history of high blood pressure, diabetes, and a heart attack three years ago experienced sudden painless loss of vision in his right eye three days ago. His vision in the right eye was impaired, with only the ability to perceive hand motion, while his left eye had 20/40 vision. A test for RAPD was positive in the right eye. Upon examination, there was arcus senilis and moderate senile nuclear sclerotic cataract in both eyes. The IOP was 14 mmHg on the right and 15 mmHg on the left. A fundus examination of the right eye revealed diffuse retinal paleness, edema, and a cherry-red spot. Despite more than 18 hours passing, no intervention was performed. The OCTA scan showed a significant decrease in the retinal blood vessels in both the superficial and deep capillary plexus (Figure 2). There was no blood flow, except for minimal flow in the large vessels.
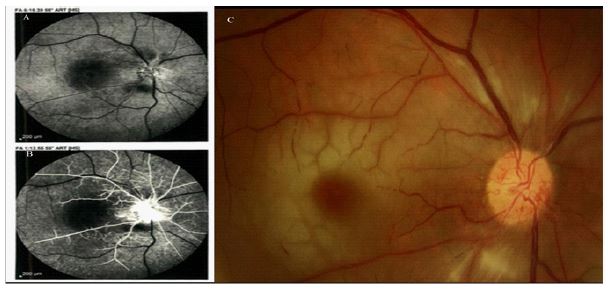
Case 3: A 62-year-old man with a history of systemic hypertension was referred with a complaint of reduced vision in his right eye that started two days ago. Following clinical and OCT findings, he was diagnosed with CRAO. His BCVA was hand motion in the right eye and 20/25 in the left eye. A positive RAPD was observed in the right eye. Anterior segment examination showed no abnormalities, and the IOP was 10 mmHg in the right eye and 11 mmHg in the left eye. Fundus examination of the right eye revealed diffuse retinal paleness and edema with a cherry-red spot.
Two weeks later, he returned with a painful eye, light perception BCVA, and an IOP of 52 mmHg in the right eye due to neovascular glaucoma. Neovascularization of the disc and pale retina was observed during the fundus exam. The fluorescein angiography showed a significant delay in the retinal circulation, retinal ischemia, and leakage from the disc neovascularization (Figure 3). Prompt full pan-retinal photocoagulation (PRP) and intravitreal Avastin (1.25 mg/0.05 ml) were performed in addition to topical anti-glaucoma medication. The IOP was under control three weeks later, and the retinal and iris neovascularization had resolved.
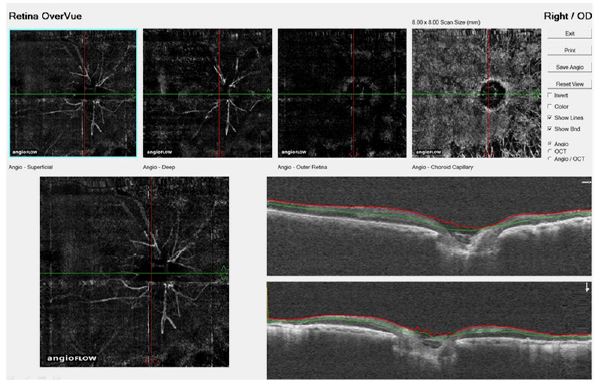
In the OCTA images, a noticeable reduction in the vascular plexus was observed in both the superficial and deep capillary layers. Blood flow was exclusively observed in the large peripapillary vessels, while the vessels in other areas appeared to be depleted. In the regions targeted for PRP treatment, there was visible atrophy of the retinal pigment epithelium, allowing the large choroid vessels to be seen (Figure 4).
Discussion
In this observational case series, we utilized OCTA to delineate RAO. In our cases, we observed a diminished vascular plexus in both the superficial and deep capillary layers. OCTA indicated a lack of flow in the foveal and perifoveal areas in both the SCP and DCP. However, we noted minimal alteration in choriocapillaris and choroidal vascular flow.
Retinal arterial occlusion is a relatively rare clinical condition but is more prevalent among the elderly. It can be caused by various factors, including cholesterol emboli, Hollenhorst plaques originating from carotid atheromatous plaques, platelet-fibrin, and calcific emboli [5]. Atherosclerotic thrombosis at the level of the lamina cribrosa is the primary cause in most cases of CRAO. This can be compromised by embolization, hemorrhage, thrombosis, arterial spasm, aneurysmal dissection, and other factors [6].
The diagnosis of CRAO relies on clinical assessment, but imaging techniques can be utilized to confirm the diagnosis, evaluate the extent of involvement, and determine the prognosis. Conventional fluorescein angiography can reveal reduced blood flow in the occluded vessel territory and inner retinal edema and opacification in inner retinal layers when examined using SD-OCT [7].
OCTA, a rapid and non-invasive imaging technique, assesses the decorrelation between two consecutive OCT images and can detect blood flow through the retinal and choroidal plexuses without requiring intravenous dye injection [8]. OCTA also enables differentiation between superficial and deep retinal vasculature. This depth-resolution imaging technique provides valuable insights into various retinal and choroidal diseases inaccessible through other diagnostic modalities, such as fluorescein angiography [4]. Additionally, OCTA en face images can help identify the specific retinal capillary layer with vascular abnormalities and pinpoint the site of reduced blood flow, in contrast to conventional angiography [9].
Conclusion
In conclusion, we have documented three RAO cases using OCTA. Our findings indicate that this non-invasive and rapid imaging technique provides a more precise visualization of non-perfused areas within the retinal vascular layers, encompassing both the superficial and deep capillary plexuses.
Declarations
Financial disclosure: No author has a financial or proprietary interest in any material or method mentioned.
Ethics approval and consent to participate: All the cases were completely notified about the procedure, and signed the written informed consent. This report was approved by Committee of Ethics in Human Research at Mashhad University of Medical Sciences.
Consent for publication: Not applicable.
Availability of data and material: The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Competing interests: The authors declare that they have no competing interests.
Funding: The authors received no funding. It is the authors’ own work, not funded by government or academicals institutes.
Authors’ contributions: All the authors contributed significantly to this case report, and all authors agree to be accountable for all aspects of the work. All authors contributed equally in acquisition of clinical data about the patient and preparing the draft of the manuscript. All authors read and approved the final manuscript.
Acknowledgement: The authors would like to thank Roghayeh Shafei BA & Alireza Haddadpour BSc, Audiovisual Department, Farabi Eye Hospital, for their help in the process of this report. It is a pleasure for us to appreciate kindness of Capt. Mehdi Madadi.
References
- Hayreh SS. Central retinal artery occlusion. Indian J Ophthalmol. 2018; 66(12): 1684-94.
- Campbell JP, Zhang M, Hwang TS, Bailey ST, Wilson DJ, Jia Y, et al. Detailed Vascular Anatomy of the Human Retina by Projection-Resolved Optical Coherence Tomography Angiography. Sci Rep. 2017; 7: 42201.
- Cugati S, Varma DD, Chen CS, Lee AW. Treatment options for central retinal artery occlusion. Curr Treat Options Neurol. 2013; 15(1): 63-77.
- de Carlo TE, Romano A, Waheed NK, Duker JS. A review of optical coherence tomography angiography (OCTA). Int J Retina Vitreous. 2015; 1: 5.
- Varma DD, Cugati S, Lee AW, Chen CS. A review of central retinal artery occlusion: clinical presentation and management. Eye. 2013; 27(6): 688.
- Cho KH, Ahn SJ, Cho JH, Jung C, Han MK, Park SJ, et al. The Characteristics of Retinal Emboli and its Association with Vascular Reperfusion in Retinal Artery Occlusion. Invest Ophthalmol Vis Sci. 2016; 57(11): 4589-98.
- Rim TH, Han J, Choi YS, Hwang SS, Lee CS, Lee SC, Kim SS. Retinal Artery Occlusion and the Risk of Stroke Development: Twelve-Year Nationwide Cohort Study. Stroke. 2016; 47(2): 376-82.
- de Castro-Abeger AH, de Carlo TE, Duker JS, Baumal CR. Optical Coherence Tomography Angiography Compared to Fluorescein Angiography in Branch Retinal Artery Occlusion. Ophthalmic Surg Lasers Imaging Retina. 2015; 46(10): 1052-4.
- Yu S, Pang CE, Gong Y, Freund KB, Yannuzzi LA, Rahimy E, et al. The spectrum of superficial and deep capillary ischemia in retinal artery occlusion. Am J Ophthalmol. 2015; 159(1): 53-63.e1-2.