
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Ophthalmoplegia in a patient with arthrogryposis multiplex congenita 3: A case report and review of literature
Mohammad Yaser Kiarudi; Saeed Shokouhi Rad; Seyed Hosein Ghavami Shahri; Mohammad Reza Ansari Astaneh; Hamid Reza Heidarzadeh*
Eye Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
*Corresponding Author : Hamid R Heidarzadeh
Eye Research Center, Khatam-al-Anbia Eye Hospital, Qarani Blvd, Mashhad University of Medical Sciences, Mashhad, Iran.
Tel: +98-51- 37245363, Fax: +98-51- 37285290;
Email: dr.hamidreza.heidarzade@gmail.com
Received : May 26, 2024
Accepted : Jun 10, 2024
Published : Jun 17, 2024
Archived : www.jcimcr.org
Copyright : © Heidarzadeh HR (2024).
Abstract
Objective: To report a patient with Arthrogryposis Multiplex Congenita (AMC) 3, myogenic type, presented with external ophthalmoplegia.
Case report: A thirteen-year-old boy with AMC from Mashhad was referred to our pediatrics ophthalmology clinic with gradual onset, bilateral upper eyelid ptosis for six months, which worsened one month ago. His parents were relatives, and a whole-exome sequencing test revealed a homozygous likely pathogenic variant in the SYNE1 gene. The best-corrected visual acuity was 20/20 in both eyes. His bilateral upper eyelid ptosis, elevation limitation in both eyes, and strabismus examinations revealed a small-angle intermittent exotropia. A slit-lamp and fundus examination of both eyes revealed no pathologic findings. He is under observation.
Conclusion: In this report, a patient with AMC developed progressive bilateral upper eyelid ptosis and elevation limitation of both eyes. It may be the start of chronic progressive ophthalmoplegia.
Keywords: Chronic progressive external ophthalmoplegia; Arthrogryposis multiplex congenita 3; Case report
Citation: Kiarudi MY, Rad SS, Shahri SHG, Astaneh MRA, Heidarzadeh HR. Ophthalmoplegia in a patient with arthrogryposis multiplex congenita 3: A case report and review of literature. J Clin Images Med Case Rep. 2024; 5(6): 3126
Introduction
Arthrogryposis Multiplex Congenita (AMC) is a group of genetically heterogeneous disorders characterized by a reduced fetal movement that develops congenital joint contracture. Its prevalence is less than one in a million [1]. Myogenic-type AMC 3 has been described as an autosomal recessive disease that can be secondary to mutations of the SYNE-1 gene [2]. It causes variable skeletal defects, including clubfoot and scoliosis, motor development delay, facial weakness, absent deep tendon reflexes, and normal motor and sensory nerve conduction [3]. Chronic Progressive External Ophthalmoplegia (CPEO) indicates a wide range of etiologies. It is characterized by painless, bilateral, and mainly symmetric ptosis and ocular motility deficit [4]. This report presents a young boy with confirmed autosomal recessive myogenic type AMC 3 who is developing CPEO.
Case report
A thirteen-year-old boy with AMC was referred to our pediatrics ophthalmology clinic with gradual onset, bilateral upper eyelid ptosis for six months, which worsened one month ago. He was from Mashhad, and his parents were relatives. He was a full-term normal vaginal delivery with a birth weight of 3800 gr. He had a history of congenital musculoskeletal disorder with scoliosis, four limb deformities, and difficulty walking since birth. He was using braces for his club foot. He had a masked face.
A whole-exome sequencing test revealed a homozygous likely pathogenic variant in the SYNE1 gene, which confirmed the AMC 3, myogenic type diagnosis. His parents were heterozygous for the same variant. IQ and mental development were normal. The nerve conduction velocity test demonstrated no pieces of evidence of neuropathy, demyelination, or axonopathy and was normal. Electromyography showed myopathic changes in the character of the motor unit potentials.
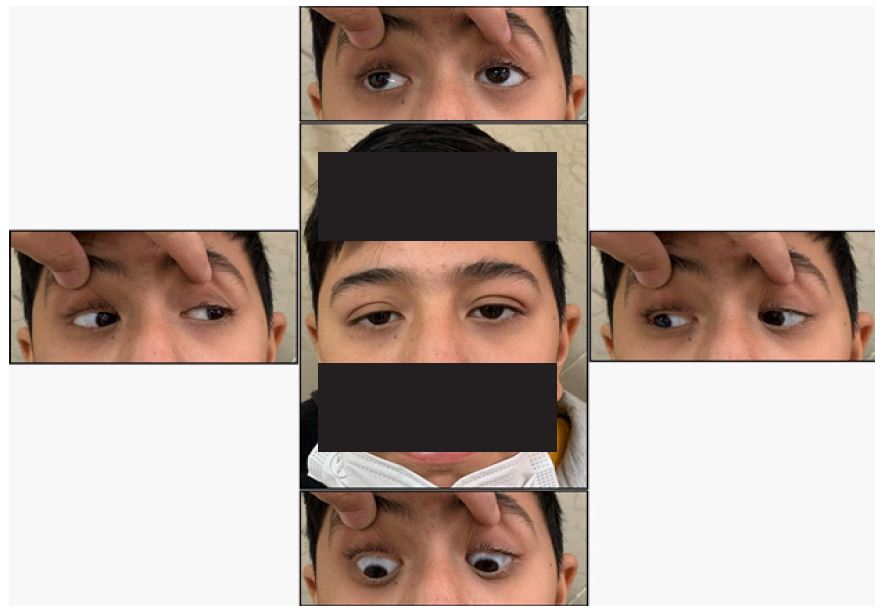
Table 1: Ocular manifestations in Arthrogryposis Multiplex Congenita (AMC).
| Ophthalmic manifestation | Number of cases | Refrences |
|---|---|---|
| Moebius syndrome | 15 | 14-22 |
| Hypertelorism | 12 | 21, 23, 24 |
| Microphthalmia | 9 | 21, 25 |
| Glaucoma | 6 | 6, 11, 12, 21, 26 |
| Extraocular muscle palsy and strabismus | 6 | 6-8, 10, 17, 27 |
| Optic nerve atrophy | 3 | 28, 29 |
| Cataract | 2 | 21, 26 |
| Neurotrophic keratitis | 2 | 13 |
| Lid abnormality | 1 | 30 |
The best-corrected visual acuity was 20/20 in both eyes with no significant refraction, and both eyes’ intra-ocular pressure was in normal ranges. Pupil examination was normal, and the relative afferent pupillary defect was absent. The patient had bilateral upper eyelid ptosis with good levator function. Extraocular muscle examination demonstrated elevation limitation in both eyes, and strabismus examinations revealed a small-angle intermittent exotropia about ten prism diopter for far and near measurements (Figure 1). Slit-lamp and fundus examination of both eyes revealed no pathologic findings. With a possible diagnosis of early CPEO, the patient is under observation.
Discussion
Herein, we reported a case of AMC with bilateral progressive ptosis, elevation limitation in ocular motility, and a small-angle intermittent exotropia, which we think may be the early stage of CPEO. Nesprin 1 is one of the nuclear membrane proteins that contribute to the nuclear architecture and cytoplasm linkage and is encoded by SNE1. The larger isoforms of this protein localize to the sarcomere in skeletal muscle. Mutations of nesprin are known to cause Emery-Dreifuss muscular dystrophy and AMD 3 [5].
Ophthalmological findings in AMC have been described previously. Zeiter et al. reported a case of AMC with congenital ophthalmoplegia and juvenile-onset glaucoma, which was extremely difficult to treat surgically [6]. Paez et al. reported a case of AMC with progressive lateral rectus paresis and deterioration of the visual evoked responses with preservation of normal ERG responses [7]. Puri et al. reported an eleven-year-old boy with an initiall abduction limitation of the left eye, followed by adduction limitation, and considered Duane’s retraction syndrome. Finally, the diagnosis of progressive ophthalmoplegia was made due to progressive loss of elevation and depression. They also suggest that previous reports on the association of AMC and lateral rectus palsy or Duane’s syndrome might be the sequential stages of ophthalmoplegia [8].
Sharma et al. in a review of literature on ophthalmological manifestations in AMC, found 14 cases with Moebius syndrome, 11 cases with hypertelorism, nine cases with microphthalmia, three cases with congenital glaucoma, two cases of congenital cataract, two cases of lateral rectus palsy, and one with Duane’s syndrome [9]. Also, we found some cases of lid abnormalities, optic atrophy, Peter’s anomaly, corneal opacity with peripheral anterior synechiae, and goniodysgenesis among AMC patients [9,13].
In the literature review, we summarized the reported ophthalmic manifestations of arthrogryposis in Table 1. The most reported ophthalmic findings were Moebius syndrome, hypertelorism, and microphthalmia [14,24]. Congenital glaucoma has been reported, demonstrating the necessity of checking intraocular pressure and optic nerve examination in infants with AMC [11,12,21,26]. Also, we suggest follow-up visits to detect juvenile-onset glaucoma [6]. On the other hand, the fundus examination can reveal optic nerve atrophy [28,29]. Extraocular muscle palsy and strabismus cases have been reported, and the onset time is usually in the late first decade and early second decade of ages [6,8,10,17,27]. Other reported ocular findings are cataracts, keratitis, and lid abnormalities [13,21,26,30].
Here we reported a young boy with AMC 3 who developed ptosis and elevation limitation in the setting of probable progressive ophthalmoplegia. In conclusion, ophthalmoplegia could happen in AMC. Regarding accumulating evidence, AMC could be considered a new etiology for CPEO.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Consent for publication was acquired from patient and his parents.
Availability of data and materials: The datasets used during the current study are available from the corresponding author on reasonable request.
Competing interests: The authors declare that they have no competing interests.
Funding: The authors received no funding. It is the authors’ work, not funded by the government or academic institutes.
Authors’ contributions: All the authors contributed significantly to this report, and all authors agree to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Acknowledgments: None.
References
- Attali R, Warwar N, Israel A, et al. Mutation of SYNE-1, encoding an essential component of the nuclear lamina, is responsible for autosomal recessive arthrogryposis. Hum Mol Genet. 2009; 18(18): 3462-3469. doi:10.1093/hmg/ddp290.
- Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015; 17(5): 405-424. doi:10.1038/gim.2015.30.
- Baumann M, Steichen-Gersdorf E, Krabichler B, et al. Homozygous SYNE1 mutation causes congenital onset of muscular weakness with distal arthrogryposis: a genotype-phenotype correlation. Eur J Hum Genet. 2017; 25(2): 262-266. doi:10.1038/ejhg.2016.144.
- Lee AG, Brazis PW. Chronic progressive external ophthalmoplegia. Curr Neurol Neurosci Rep. 2002; 2(5): 413-417. doi:10.1007/s11910-002-0067-5.
- Sweet ME, Taylor MRG, Mestroni L. Diseases of the nuclear membrane. In: Jeffries JL, Blaxall B, Robbins J, Towbin JA, editors. Cardioskeletal myopathies in children and young adults. London: Academic Press; 2017; 233-48.
- Zeiter JH, Boniuk M. Ophthalmologic findings associated with arthrogryposis multiplex congenita: case report and review of the literature. J Pediatr Ophthalmol Strabismus. 1989; 26(4): 204-208. doi:10.3928/0191-3913-19890701-11.
- Paez JH, Tuulonen A, Yarom R, Arad I, Zelikovitch A, BenEzra D. Ocular findings in arthrogryposis multiplex congenita. J Pediatr Ophthalmol Strabismus. 1982; 19(2): 75-79. doi:10.3928/0191-3913-19820301-04.
- Puri P, Gupta M, Chan J. Progressive ophthalmoplegia in arthrogryposis multiplex congentia. Eye (Lond). 2002; 16(1): 86-88. doi: 10.1038/sj.eye.6700014.
- Sharma R, Sharma P, Raina J. Ophthalmological and systemic findings associated with arthrogryposis multiplex congenita. Internet J Trop Med. 2006; 3.
- Anilkumar ES, Narendran K. Ocular findings associated with arthrogryposis multiplex congenita. Indian J Ophthalmol Case Rep. 2021; 1: 444. doi: 10.4103/ijo.IJO_192_21.
- Kulkarni MV, Panjabi M. Congenital glaucoma--an association with arthrogryposis multiplex congenita--a case report. Indian J Ophthalmol. 1988; 36(4): 179-181.
- Sakamoto T, Tawara A, Inomata H. Goniodysgenesis of the eye with arthrogryposis multiplex congenita. Ophthalmologica. 1992; 204(4): 210-214. doi:10.1159/000310296.
- Brooks JG Jr, Coster DJ. Arthrogryposis multiplex congenita: a report of two cases. Aust N Z J Ophthalmol. 1994; 22(2): 127-132. doi:10.1111/j.1442-9071.1994.tb00780.x.
- Henderson JL. The congenital facial diplegia syndrome: clinical features, pathology and aetiology: a review of sixty-one cases. Brain. 1939; 62(4): 381-403.
- Sprofkin BE, Hillman JW. Moebius’s syndrome; congenital oculofacial paralysis. Neurology. 1956; 6(1): 50-54. doi:10.1212/wnl.6.1.50.
- Van Allen MW, Blodi FC. Neurologic aspects of the Mobius syndrome. A case study with electromyography of the extraocular and facial muscles. Neurology. 1960; 10: 249-259. doi:10.1212/wnl.10.3.249.
- Wishnick MM, Nelson LB, Hupport L, Reich EW. Moebius syndrome with limb abnormalities with dominant inheritance. Ophthalmic Paediatr Genet. 1983; 2: 77-81. doi: 10.3109/13816818309007794.
- Hanissian AS, Fuste F, Hayes WT, Duncan JM. Möbius syndrome in twins. Am J Dis Child. 1970; 120(5): 472-475. doi:10.1001/archpedi.1970.02100100136020.
- Baraitser M. Genetics of Möbius syndrome. J Med Genet. 1977; 14(6): 415-417. doi:10.1136/jmg.14.6.415.
- Drachman DB, Banker BQ. Arthrogryposis multiplex congenita. Case due to disease of the anterior horn cells. Arch Neurol. 1961; 5: 77-93. doi:10.1001/archneur.1961.00450130079010.
- Banker BQ. Arthrogryposis multiplex congenita: spectrum of pathologic changes. Hum Pathol. 1986; 17(7): 656-672. doi:10.1016/s0046-8177(86)80177-0.
- Moreira AT, Teixeira S, Ruthes HI, Miranda AB, Guerra DR. Moebius syndrome associated with arthrogryposis: case report and literature review. Arquivos Brasileiros de Oftalmologia. 2001; 64: 576-9.
- Labrune M. Lefebre J. Donnees de Fexamen electromyographique au cours des arthrogryposis. Rev Neurol. 1963; 108: 209-211.
- Tabet AC, Aboura A, Gérard M, et al. Molecular characterization of a de novo 6q24.2q25.3 duplication interrupting UTRN in a patient with arthrogryposis. Am J Med Genet A. 2010; 152A(7): 1781-1788. doi:10.1002/ajmg.a.33433.
- Hall JG. Nicht-chrmosomal bedingte Dysmophie-Syndrome. Klin Gen Paediatr. Mainz Symposion.1980; 1: 105-121.
- Swinyard CA, Mayer V. Multiple congenital contractures. Public health considerations of arthrogryposis multiplex congenita. JAMA. 1963; 183: 23-27.
- Krieger I, Espiritu CE. Arthrogryposis multiplex congenita and the Turner phenotype. Am J Dis Child. 1972; 123(2): 141-144. doi:10.1001/archpedi.1972.02110080119014.
- Fowler M. Arthrogryposis multiplex congenita. Arch Dis Child. 1959; 34: 505-10.
- Fukumura S, Ohba C, Watanabe T, et al. Compound heterozygous GFM2 mutations with Leigh syndrome complicated by arthrogryposis multiplex congenita. J Hum Genet. 2015; 60(9): 509-513. doi:10.1038/jhg.2015.57.
- Margolis S, Luginbehul B. Eye abnormalities associated with Arthrogryposis multiplex congenital. J Pediatr Ophthalmol. 1975; 12: 57-60.