
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A case report on superior mesenteric artery or Wilkie’s syndrome
Tejas Falke1*; Roshni Warghane2; Jaya Khandar3
1Basic BSC Nursing 4 Year, Smt. Radhikabai Meghe Memorial College of Nursing, Sawangi (Meghe), Wardha, Datta Meghe Institute of Medical Sciences (Deemed to Be University) Maharashtra, India.
2Assistant Professor, Department of Obstetrics & Gynecology Nursing, Smt. Radhikabai Meghe Memorial College of Nursing, Sawangi (Meghe), Wardha, Datta Meghe Institute Medical Sciences (Deemed to Be University) Maharashtra, India.
3Assistant Professor, Department of Community Health Nursing, Smt. Radhikabai Meghe Memorial College of Nursing, Sawangi (Meghe), Wardha, Datta Meghe Institute Medical Sciences (Deemed to Be University) Maharashtra, India.
*Corresponding Author : Tejas Falke
Basic BSC Nursing 4 Year, Smt. Radhikabai Meghe Memorial College of Nursing, Sawangi (Meghe), Wardha, Datta Meghe Institute of Medical Sciences (Deemed to Be University) Maharashtra, India.
Email: Tejasfalke55@gmail.com
Received : May 26, 2024
Accepted : Jun 11, 2024
Published : Jun 18, 2024
Archived : www.jcimcr.org
Copyright : © Falke T (2024).
Abstract
Superior Mesenteric Artery Syndrome (SMAS), often known as Wilkie’s syndrome, is a rare clinical phenomenon brought on by the duodenum’s third segment being squeezed in between the abdominal aorta and superior mesenteric artery, resulting in acute starvation and intestinal blockage. The authors report a case of a male patient with 30 years old of chronic intestinal obstruction with abdominal pain, vomits and weight loss. Contrast intestinal series showed dilation of stomach and duodenum. An abdominal computed CT scan were consistent with SMAS. He received basic nutritional care and underwent a successful laparoscopic duodenojejunostomy procedure. Most instances of SMAS with persistent symptoms or ineffectiveness of conservative therapy may require surgery. A minimally invasive surgical technique is a safe surgical alternative with good results. The discussion includes clinical specifics, diagnostic tests, and therapy. The management of this condition varies between observation and surgery, based on each unique situation. The main therapeutic approach was given the patient he was treated surgical operation and antibiotics anti-emetics during hospitalization.
Keywords: Superior Mesenteric Artery (SMA); Wilkies syndrome; Intestinal obstruction; Weight loss.
Citation: Falke T, Warghane R, Khandar J. A case report on superior mesentreric artery or Wilkie’s syndrome. J Clin Images Med Case Rep. 2024; 5(6): 3127.
Introduction
A proximal intestinal obstruction can pose complexity of the gastrointestinal system, doctors may encounter difficulties in diagnosing a proximal intestine blockage. A gastrointestinal blockage that presents in an uncommon way and causes a variety of symptoms is known as Superior Mesenteric Artery syndrome (SMA syndrome). Persistent ileus of the stomach, cast syndrome, or vascular duodenal compression [1]. Because Wilkie’s 1927 depiction was the first in-depth account, only few In the medical literature, instances have been documented. An unsuspecting physician may face a diagnostic conundrum due to its uncommon nature and non-pathognomonic symptomatology [2] has an estimated incidence of 0.013%-0.3% and just 500 documented instances in the literature, making it very uncommon. The Austrian scholar Carl Freiherr von Rokitan-sky initially reported SMA disease in 1861 as a result of an autopsy [3]. Eventually, Wilkie offered a more thorough clinical and pathophysiologic explanation in a group of 64 individuals along with recommended therapeutic strategies. Following that, there was debate over whether this syndrome actually exists, particularly in light of the symptoms’ lack of specificity and the extensive number of possible diagnoses. But improvements in imaging technologies, such magnetic resonance imaging and Computed Tomography (CT), have made it moreeasier to see the angle between the aorta and the SMA clearly, which has increased the diagnosis rate.
Patients may present symptoms are gastrointestinal obstruction, generalized weakness & vomiting after meal 1 month such as with recurrent episodes upper abdominal distension and epigastric tenderness [4]. Therefore, a thorough medical history along with imaging results should strongly suggest the diagnosis of SMA syndrome in the right clinical setting. A number of complications, including electrolyte imbalance, catabolic wasting, peritonitis, and gastrointestinal perforation, might result from delaying this diagnosis. He was incorrectly diagnosed with an eating disorder and obtained treatment.
Upper gastrointestinal contrast study and contrast-enhanced CT abdomen are used to confirm the diagnosis, which is essentially made by ruling out other possible causes of upper GI blockage. All patients can have an initial conservative therapy trial, but duodenojejunostomy surgery provides early and thorough symptom alleviation. Nonetheless, after a CT scan, Wilkie’s syndrome was confirmed to the endoscopy ultrasonography & common investigation are CBC, KFT, LFT and URINE TEST. He undergone one surgery and completely he was recovered [5].
Case presentation
A 30 year-old adult male was brought to the surgery OPD in an conscious state with a complete of pain in abdomen after taking a meal, vomiting after meal since 1 month, generalized weakness H/O fever cough 4 days back. Primary prevention measure were taken by the doctor her patient state that severe pain in abdomen. The primary visit the private hospital the physical examination and reffered to the multispecialty hospital.
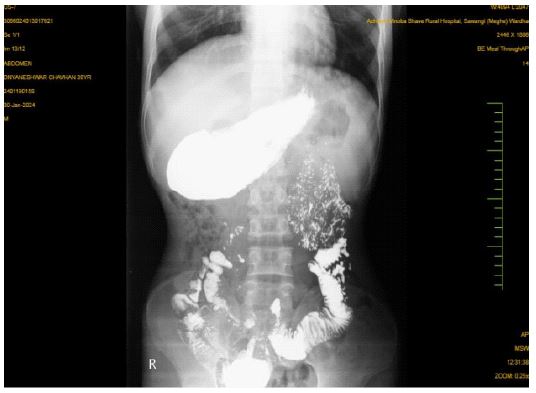
On the physical examination swelling and tenderness of the abdomen bowel sound check they are abnormal tachycardia bradypnea. The vital sign are cheeked they are heart rate are 90 bpm were essential CT-SCAN and ULTRASONOGRAPHY & ENDOSCOPY are done CT-scan are report there is gross dilatation of stomach multiple metopic artifact noted in region of pylorus leading to suboptimal evaluation D1 and D2 segment of duodenum appears prominent and narrowing D3 segment. USG report are there is c/o compression of 3rd part of duodenum between SMA & aorta of 2.5 mm is diagnosed of SMA. Endoscopy report: Pyloric stricture (CRE balloon dilatation done) tight duodenal stricture the patient was moved to the male surgery ward for further management.
The patient was prepared the operation are open gastrojejunoctomy they are done simultaneously the patient was administered 500 ml RL and inj. cefotaxime 1 mg, inj. Metronidazole 100 ml on laboratory investigation, complete blood count and were all within normal range. On fifth day hospitalization patient vital sign may be stable. Medical management continued and patient prognosis and suture are heal.

Discussion
SMAS is an uncommon condition described as a compression of the third segment of the duodenum between the SMA and AA resulting in partial or total duodenal blockage. It is also referred to as Wilkie’s syndrome, mesenteric duodenal compression syndrome, chronic duodenal ileus, or cast syndrome. When the duodenum’s third segment is compressed in between the SMA and the aorta, Wilkie’s syndrome are develops [6]. The angle that typically exists between the aorta and SMA is between 25° and 60°, but in this syndrome it is constricted. Congenital defects, severe weight loss, lumbar hyperlordosis, and restorative proctocolectomy with ileal-anal anastomosis can all cause the aortomesenteric angle to narrow. The reported incidence of SMA syndrome is thought to be between 0.01% and 0.3% because of the condition’s uncommon appearance. Females are 1.5 times more likely than men to acquire it, and it has been seen more frequently in young people in their first and fourth decades of life. Then then, it may happen at any age [7]. There is currently no known racial or ethnic predilection. The estimated prevalence of SMAS in the general population ranges from 0.3% to 0.013, with females aged 10 to 40 being the most typically affected [8]. Its symptoms are multifaceted and include early satiety, weight loss, nausea, vomiting, postprandial epigastric discomfort, and malnourishment. SMAS might manifest as an immediate blockage or develop slowly over time with persistent symptoms. Individuals suffering with SMA syndrome may exhibit acute symptoms, persistent but subtle symptoms over time, or an intense flare-up of long-term symptoms. Duodenal blockage symptoms and indications are often associated with acute presentation [9]. Patients with chronic conditions, such as our patient, may exhibit persistent, nonspecific stomach discomfort or recurring bouts of abdominal pain accompanied by vomiting. Gastric distension, early satiety with a feeling of fullness due to an extended gastroduodenal transit time, and esophageal reflux are other, less prevalent symptoms. The diagnosis of SMA syndrome is extremely difficult because of its sneaky start [10]. We could determine the correct diagnosis based on the patient’s clinical presentation, medical history, and imaging testing. Barium tests may demonstrate sluggish gastroduodenojejunal transit together with duodenal and possibly stomach dilatation. An extrinsic compression and constriction at the level of the third section of the duodenum may be seen during an endoscopy. An accurate assessment of the aortomesenteric angle and distance, as well as sufficient imaging of the duodenum’s vascular compression, are made possible by contrast-enhanced CT or magnetic resonance angiography. This information is highly helpful for both diagnostic and surgical treatment planning. SMA syndrome is managed according to an individual’s needs, using either invasive therapy or conservative treatment along with nutritional assistance. It’s essential to use multidisciplinary management [11]. Psychotherapy is a crucial component of treatment, along with educating patients about lifestyle modifications, because mental illness and nutritional disorders are commonly associated. Due to their large weight reduction, the majority of patients need nutritional consultations as well as close clinical follow-ups with nutritionists and gastroenterologists. The principal benefits of this approach include a shorter surgical duration, little blood loss, reduced discomfort after surgery, minimal danger of adhesions after surgery, good esthetic results, early bowel peristalsis recovery, decreased risk of incisional hernia, and a shorter hospital stay [12]. In conclusion, surgery should be considered if there are multiple symptoms and indicators, such as the presence of complications, a refractory response to conservative medical management, and a prolonged duration of severe and recurrent upper gastrointestinal symptoms (at least once a week for more than six months). The Treitz Ligament Division (Strong’s Operation), gastrojejunostomy, partial gastrectomy, Billroth II gastrojejunostomy, duodenojejunostomy, anterior repositioning of the intestinal tract, circumferential draining of the duodenum, duodenal derotation, and duodenal resection are among the various surgical techniques used to treat SMAS [13]. The superior mesenteric artery transposition is another technique about which reports have been made. A duodenojejunostomy was the first surgical operation used to treat SMAS, and it was performed in 1908. For many years, it was considered the best surgical choice [14].
Conclusion
We believe the underdiagnoses of SMA syndrome. It is crucial to have a top level of clinical suspicion, particularly in individuals who are experiencing significant weight loss and stomach distension symptoms. It is also important to take surgical stress into account as a potential SMA syndrome cause. In this frequently underappreciated illness, interdisciplinary collaboration yields the best diagnostic and treatment outcomes. Finally, we want to draw attention to how challenging it may be to diagnose SMA condition accurately in an unusual clinical environment like the one we experienced. A novel treatment option that combines the well-established benefits of minimally invasive surgery for the syndrome of superior mesenteric artery compression. It is a reasonably problem-free, safe, and efficient technique that takes an appropriate amount of time to do, and it promotes a speedy recovery for the patient.
Disclosures
Human subjects: Consent was obtained or waived by all participants in this study.
Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work.
Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
References
- Cureus | Perplexing Case of Wilkie’s Syndrome: A Rare Presentation in a Young Patient | Available from: https://www.cureus.com/articles/21233-perplexing-case-of-wilkies-syndrome-a-rare-presentation-in-a-young-patient#!/.
- 13.pdf Available from: https://www.jcpsp.pk/archive/2011/Jan2011/13.pdf.
- Wilkie’s syndrome prevalence - Google Search Available from: https://www.google.com/search?q=wilkie%27s+syndrome+prevalence&source=lmns&bih=632&biw=641&hl=en&sa=X&ved=2ahUKEwj_
2Ork59KEAxVeTGwGHYh8CtkQ0pQJKAB6BAgBEAI. - Kefeli A, Aktürk A, Aktaş B, Çalar K. Wilkie’s Syndrome: A Rare Cause Of Intestinal Obstruction. Arq Bras Cir Dig Abcd. 2016; 29(1): 68-9.
- Molina Proaño GA, Cobo Andrade MM, Guadalupe Rodríguez RA, Gálvez Salazar PF, Cadena Aguirre DP, González Poma GV, et al. Wilkie’s syndrome, a missed opportunity. J Surg Case Rep. 2018; 2018(9): rjy246.
- Catarino Santos S, Loureiro AR, Simão R, Pereira J, Pinheiro LF, Casimiro C. Wilkie’s syndrome: a case report of favourable minimally invasive surgery. J Surg Case Rep. 2018; 2018(2): rjy027.
- KEFELI A, AKTÜRK A, AKTAŞ B, ÇALAR K. WILKIE’S SYNDROME: A RARE CAUSE OF INTESTINAL OBSTRUCTION. Arq Bras Cir Dig ABCD. 2016; 29(1): 68-9.
- Waqar SHB, Khan AA, Mohiuddin O, Waqar SHB, Khan AA, Mohiuddin O. Perplexing Case of Wilkie’s Syndrome: A Rare Presentation in a Young Patient. Cureus [Internet]. 2019; (7). Available from: https://www.cureus.com/articles/21233-perplexing-case-of-wilkies-syndrome-a-rare-presentation-in-a-young-patient
- Catarino Santos S, Loureiro AR, Simão R, Pereira J, Pinheiro LF, Casimiro C. Wilkie’s syndrome: a case report of favourable minimally invasive surgery. J Surg Case Rep. 2018; 2018(2): rjy027.
- Zaraket V, Deeb L. Wilkie’s Syndrome or Superior Mesenteric Artery Syndrome: Fact or Fantasy. Case Rep Gastroenterol. 2015; 9(2): 194-9.
- Requena-López AA, Mata-Samperio BK, Cuadra-Reyes LA, Casillas-Vargas R, Requena-López AA, Mata-Samperio BK, et al. Wilkie’s syndrome as a cause of bowel obstruction in adults: A case report. Cir Cir. 2020; 88(2): 185-8.
- Apostu RC, Chira L, Colcear D, Lebovici A, Nagy G, Scurtu RR, et al. Wilkie’s syndrome as a cause of anxiety-depressive disorder: A case report and review of literature. World J Clin Cases. 2022; 10(5): 1654-66.
- Ushiki A, Koizumi T, Yamamoto H, Hanaoka M, Kubo K, Matsushita M. Superior mesenteric artery syndrome following initiation of cisplatin-containing chemotherapy: a case report. J Med Case Reports. 2012; 6(1): 14.
- Matheos E, Vasileios K, Ioannis B, Dimitrios Z, Kostas H. Superior Mesenteric Artery Syndrome. Case Rep Gastroenterol. 2009; 3(2): 156-61.