
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Pure colloid carcinoma of the breast: About a rare case
Aggoug Zine Elabidine*; El Karoini Doha1; Bencherifi Y2; Ennachit M2; Benhessou M2; El Kerroumi M3
1Resident Doctor in Obstetrics and Gynecology Department, University Hospital Center Ibn Rochd, Casablanca, 20100, Morocco.
2Professor in Obstetrics and Gynecology Department, University Hospital Center Ibn Rochd, Casablanca, 20100, Morocco.
3Head of Service in Obstetrics and Gynecology Department, University Hospital Center Ibn Rochd, Casablanca, 20100, Morocco.
*Corresponding Author : Aggoug Z Elabidine
Resident Doctor in Obstetrics and Gynecology Department, University Hospital Center Ibn Rochd, Casablanca, 20100, Morocco.
Tel: 00212-653413071;
Email: aggoug.zine@gmail.com
Received : May 28, 2024
Accepted : Jun 11, 2024
Published : Jun 18, 2024
Archived : www.jcimcr.org
Copyright : © Elabidine AZ (2024).
Abstract
Introduction: Colloid carcinoma of the breast, also known as mucinous or gelatinous carcinoma, is a rare histological form of cancer. It is characterized by the production of extracellular mucus. Two types of colloid carcinoma are distinguished: Pure colloid carcinoma, and mixed colloid carcinoma.
Presentation of case: We report a rare case of a 48-year-old patient with a history of infiltrating carcinoma of the left breast, treated with surgery, radiotherapy, chemotherapy, and hormonal therapy in 2013, presented with pure mucinous colloid carcinoma of the right breast for which she underwent a lumpectomy with axillary dissection, radiotherapy is planned.
Discussion: The distinction between pure and mixed colloid carcinoma is significant because it determines the therapeutic approach and prognostic impact. The prognosis for the mixed form, which closely resembles invasive ductal carcinomas, is bleaker compared to the pure form. Overall survival for women with mucinous carcinoma is better than that for infiltrating carcinoma, underscoring the importance of accurate diagnosis. Surgery remains the most effective first-line treatment for managing these cancers.
Conclusion: The overall survival of women with mucinous carcinoma is better than that of infiltrating carcinoma. Surgery remains the best first-line treatment.
Keywords: Colloid carcinoma; Surgery; Case report.
Citation: Elabidine AZ, Doha EK, Bencherifi Y, Ennachit M, Benhessou M, et al. Pure colloid carcinoma of the breast: About a rare case. J Clin Images Med Case Rep. 2024; 5(6): 3128.
Introduction
Mucinous Carcinoma (MC) of the breast or colloid carcinoma is a rare histological form, accounting for 1 to 6% of all infiltrating carcinomas of the breast [1]. According to the World Health Organization (WHO), it is defined by the presence of malignant mucus-secreting tumor cells floating in mucus. Most authors agree in distinguishing two types of colloid carcinoma: pure colloid carcinoma, in which there is no or a minority ≤10% infiltrating ductal carcinoma component, and mixed colloid carcinoma, which associates foci of infiltrating ductal carcinoma alongside the colloid component [2]. This subdivision is justified by the prognosis: the pure form is characterized by the presence of tumor tissue surrounded by abundant extracellular mucus, forming a mechanical barrier that attenuates cell invasion, making this form less aggressive and giving it a more favorable prognosis than the mixed form, which is similar to that of invasive ductal carcinoma [1,2]. Those case reports have been reported per the SCARE 2020 criteria [3].
Case presentation
The patient is 48 years old, single, and has a history of infiltrating breast carcinoma of the left breast, grade SBR 2, luminal profile B Her2 positive. The patient was treated in 2013 by surgery (left mastectomy with axillary courage), followed by adjuvant treatment with radiotherapy, chemotherapy, and hormonotherapy for 5 years. The patient presented with a right breast nodule measuring 4x3 cm at the junction of the upper quadrants, with no other associated signs, notably no nipple discharge and no signs of inflammation (Figure 1).
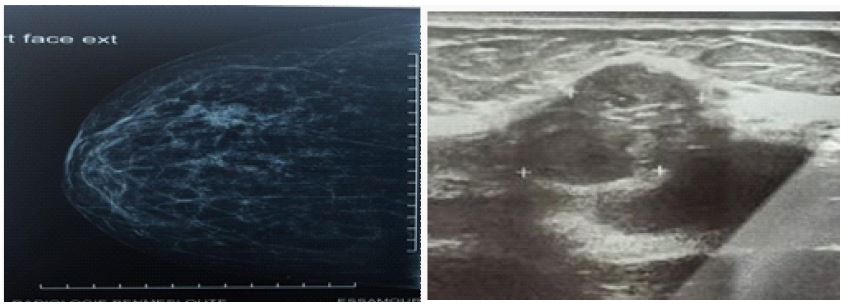
Mammo-echography revealed a coarsely rounded, well-limited, micro-lobulated, hypoechoic formation straddling the right upper quadrants, measuring 20x14 mm. A contiguous, oval, fairly well-limited, lobulated, hypoechoic formation, surrounded by a hyperechoic halo, measures 14x10.4 mm. In the left breast, there was no detectable nodular or cystic lesion opposite the mastectomy scar, and the left axillary fossa was free. The examination was classified as ACR BIRADS 4 on the right (Figure 2).
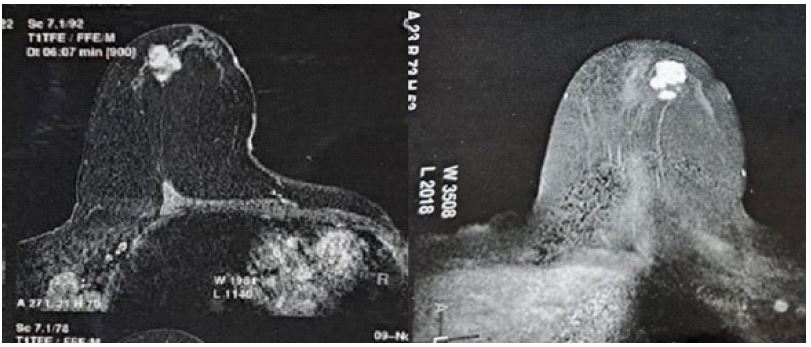
A breast MRI revealed two contiguous lesions in the upper quadrants of the right breast, with lobulated contours measuring 17x15 mm and 20x18 mm, hypo signal T1, hyper signal T2, and intense contrast after gadolinium injection. Axillary prolongation is normal. On the left, there were no notable anomalies (Figure 3).
Microbiopsy of the nodule showed pure, infiltrating mucinous colloid carcinoma, without vascular emboli. conservative surgery was performed (right lumpectomy with axillary dissection), with the pathological study of a pure mucinous carcinoma, grade SBR I, measuring 1.6 cm, and no carcinoma in situ. Lymph node dissection produced 8 lymph nodes, 3 of which were metastatic without vascular emboli or capsular rupture.
The tumor was classified as p T1N2Mo. Estrogen receptor labeling was 80%, progesterone receptor labeling was 100%, HER2 was negative and Ki 67 was 28%. The patient was transferred to the oncology department for radiotherapy.

Discussion
Colloid carcinoma is a relatively rare histological subtype of breast carcinoma, initially described in 1982 by Geschickter. It accounts for approximately 6% of all breast malignancies in individuals over the age of 75 and about 1% in those under 35. This rarity makes it an interesting and distinct entity within breast cancer [1,4].
In the literature, no significant difference has been found between colloid carcinoma, tubular carcinoma, and breast CCI.Pure colloid carcinomas often present as well-limited, mobile, even lobulated masses, which may thus be mistaken for benign formations; a sensation of suffering, crease or fluctuation is reported when colloid carcinomas of the breast are palpated. The average tumor diameter is 1.5 cm, with extremes ranging from 0.3 to 19 cm. The majority of tumors (96%) were TNM stage T1 or T2 [5].
On mammography, the presence of mucin translates into a relatively well-defined, low-density lobular mass. Occasionally, they may have partially faded or obscured margins. Up to 20% of lesions may be occult on mammography [1].
Calcification may be rare in pure mucinous types. On ultrasonography, mucinous carcinomas often show mixed echogenicity with mixed solid and cystic components, distal enhancement and microlobulated margins are commonly found in mucinous carcinomas. A mixed mucinous carcinoma tends to be more hypoechoic. On MRI, they are one of the few cancers to have very high signal intensity on T2-weighted images involving the mucinous component, compared with other malignant breast tumors [1,2,6].
Lymph node metastases in pure colloid carcinomas of the breast are their frequency increases with tumor size. Immunohistochemical studies of hormone receptors for estrogen and progesterone have often revealed a strong presence, particularly of estrogen (91% of cases) [7].
Treatment is based on surgery with or without adjuvant chemotherapy and hormone therapy. Conservative surgical treatment (lumpectomy) is recommended for T1 and small T2 cases, followed by radiotherapy. Partial and accelerated irradiation of the breast is currently the most recommended after conservative surgery [8,9]. Exclusive radiotherapy may be attempted in inoperable forms for local or general reasons. Poortmans reported a 70% reduction in the risk of locoregional recurrence in patients treated with irradiation, irrespective of age, tumor characteristics, and systemic administration of treatment [9].
Most authors agree on the favorable evolution of pure colloid carcinoma compared to other forms of breast malignancy, in particular ductal carcinoma. Which is by far the most common histological type [1]. The onset of metastases in pure colloid carcinomas is delayed late. The average time to metastasis is ten years [1,2].
Conclusion
The distinction between pure and mixed colloid carcinoma is an important one, as the therapeutic attitude and prognostic impact depend on it. The prognosis of the mixed form, similar to infiltrating ductal carcinomas, is poorer than that of the pure form. Overall survival of women with mucinous carcinoma is better than that of infiltrating carcinoma, and surgery remains the best 1st- line therapy.
Declarations
Patient consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor- in-Chief of this journal on request.
Ethical approval: I declare on my honor that my establishment has exempted the ethical approval.
Sources of funding: None.
Author’s contribution: All authors have read and approved the final version of the manuscript.
Conflicts of interest: The authors declare having no conflicts of interest in this article.
References
- Freddie Bray, Jacques Ferlay, Isabelle Soerjomataram, Rebecca L, Siegel, et al. Global Global cancer statistics: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. 2018.
- Liu H, Tan H, Cheng Y, Zhang X, Gu Y, et al. Imaging findings in mucinous breast carcinoma and correlating factors. Eur J Radiol. 2011; 80(3): 706-12.
- Agha RA, Franchi T, Sohrab C, Mathew G, Kirwan A, et al. The SCARE 2020 guideline: updating consensus Surgical Case Report (SCARE) guidelines. International Journal of Surgery. 2020; 84(1): 226-30.
- Ishikawa T, Hamaguchi Y, Ichikawa Y, Shimura M, Kawano N, et al. Locally advanced mucinous carcinoma of the breast with sudden growth acceleration: A case report. Jpn J Clin Oncol. 2002; 32: 64-7.
- Komenaka IK, El-tamer MB, Troxel A, Hamele-bena D, Joseph LA, et al. Pure mucinous carcinoma of the breast. Am J Surg. 2004; 187: 528-32.
- Nowak H, Mignot L, Roquancourtde A, Pierre TF, Corin A. Carcinomescolloïdes muqueux du sein. À propos de neuf cas suivis au centre des maladies du sein de l’hôpital Saint-Louis. Gynecology. 2013; 34: 431-4.
- Fentiman IS, Millis RR, Smith P, Ellul JPM, Lampejo O. Mucoid breast carcinoma: Histology and prognosis. Br J Cancer. 2007; 75: 1061-5.
- Komenaka IK, El-tamer MB, Troxel A, Hamele-bena D, Joseph LA, et al. Pure mucinous carcinoma of the breast. Am J Surg. 2014; 187: 528-32.
- Ucla L, Fenton J, Mathieu G, Vilcoq J, Bateini JP. Cancers colloïdes du sein. Intérêt de la radiothérapie. Série de 138 cas traités à l’institut Curie. Bull Cancer. 1998; 75: 783-7.