
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A rare variation of the median nerve in its course and branching: A case report and literature review
Alireza Shams1*; Ali Ramadan2; Mohammad Amin Shams3
1Department of Anatomy, Faculty of Medicine, Alborz University of Medical Sciences, Karaj, Iran.
2Faculty of Medicine, Alborz University of Medical Sciences, Karaj, Iran.
3Iran University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Alireza Shams
Department of Anatomy, Faculty of Medicine, Alborz University of Medical Sciences, Karaj, Iran.
Tel: +98-9123900319, Fax: +98-2634287311;
Email: dr.shams@abzums.ac.ir
Received : Apr 30, 2024
Accepted : Jun 13, 2024
Published : Jun 20, 2024
Archived : www.jcimcr.org
Copyright : © Shams A (2024).
Abstract
Background: The median nerve is vital for controlling hand movements. Thus, its variations are clinically important. In this report, we discuss a case of the median nerve with several anatomical variations.s
Case presentation: While dissecting a male cadaver, we observed several variations in the formation of divisions and cords of the brachial plexus. Median and musculocutaneous nerves originated from a common branch of the lateral cord. Furthermore, the median nerve ran medially throughout the brachial artery.
Conclusion: Understanding these variations is crucial because they may affect the function of the upper limb. They can also present challenges during surgical procedures.
Keywords: Brachial plexus; Cadaver; Median nerve; Variation.
Citation: Shams A, Ramadan A, Amin Shams M. A rare variation of the median nerve in its course and branching: A case report and literature review. J Clin Images Med Case Rep. 2024; 5(6): 3131.
Background
The median nerve (MN), also known as the ‘laborer’s nerve,’ [1] controls the fine movements of the hand, as it supplies most of the superficial and deep flexors of the forearm. Thus, its variations may be of utmost clinical importance. MN usually originates from the medial and lateral brachial plexus cords and covers the third segment of the axillary artery. It is composed of nerve fibers from roots C6–T1, whereas in certain individuals, nerve fibers from C5 may also be present [2]. It then continues down the upper arm without branching and passes through the forearm between the two heads of the pronator teres. The MN passes between the flexor digitorum profundus and superficialis in the forearm. Next, the MN descends deeply to the flexor retinaculum in the hand and wrist, from which it gives out its terminal branches, which include the palmar digital branches on the medial side and the recurrent motor branches on the lateral side [3]. In this report, we present a case with several abnormalities in the path and branching of the MN, which may provide insights for clinicians dealing with this region.
Case report
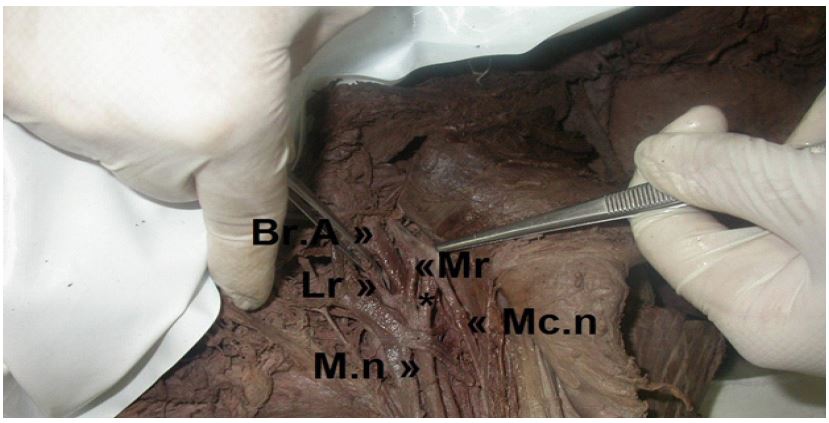
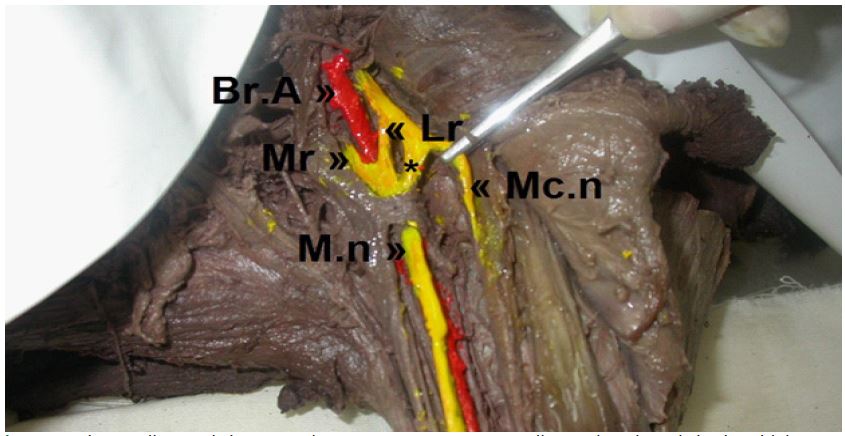
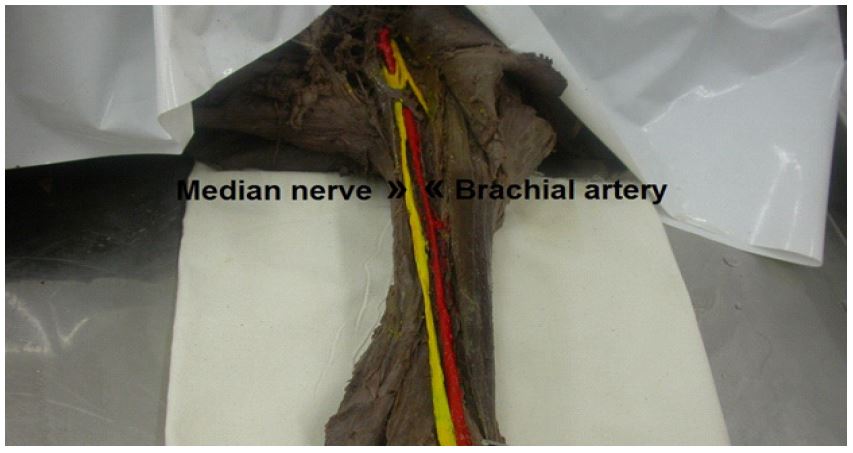
While dissecting the left brachial axillary cavity of a 60-year-old man, 168 cm tall and weighing approximately 70 kg, in the dissection hall of the Faculty of Medicine of Alborz University of Medical Sciences, which was fixed by Grant’s method [4] in 10% formalin and dissected according to Cunningham’s manual of dissection [5], several variations were observed in connection with the MN. There was a communicating branch between the lateral root of the MN and the musculocutaneous nerve (MCN) (Figure 1). Meanwhile, there was an additional communicating branch between these two nerves, which was more distal than the previous variation (Figure 2). Notably, the MN ran medially throughout the brachial artery, deviating from its typical anatomical course (Figure 3).
Discussion
Anatomical variations in the brachial plexus, such as the anastomotic branches between the MN and MCN, are not rare [6]. There have also been several attempts to classify the communicating branches between the MN and MCN. In 1998, Venieratos D et al. examined the relationship between these two nerves in 129 dissected corpses. They presented three different groups of patterns according to the location of their connection to the coracobrachialis muscle [7]. Communication in the first group occurred proximal to the MCN’s entrance into the coracobrachialis muscle, but in the second group, it occurred distal to the muscle. In the third group, neither the connecting branch nor the nerve penetrated the muscle. In this case report, the results align with a similar pattern found in the first group.
Furthermore, after dissecting 453 axillae, Maeda et al. [8] discovered that 18.8% of them had MCN communicating branches to MN (9]. In Ballesteros’ study, the arms of 53 cadavers were dissected, and in 17% of them, a communicating branch from the MCN to the MN existed [10]. In this study, the communicating branch was from the MCN to the MN.
Other types of MN variation have been reported in the forearm and carpal regions, such as high division in the MN proximal to the carpal tunnel, also referred to as a bifid MN, which was reported by Spagnoli et al. and was linked to carpal tunnel syndrome (CTS) [11]. Amadio et al. [12] also documented high bifurcation of the MN in 9 cases of carpal tunnel decompression surgery [12]. There have also been other reports of bifurcation of the MN in patients with CTS [13-15]. Trifurcation of the MN has also been observed in some cases. Lonie S et al. reported an MN trifurcation in a 32-year-old man diagnosed with CTS [16].
Furthermore, less than 50% of the 100 hands examined by Stancić et al. [17] fit the MN anatomy previously reported in the literature. To reduce the possibility of improper decompression surgery, they proposed that awareness of these abnormalities should be applied before surgery [17]. Therefore, it is believed that research in the field of pure anatomy has reached a dead end, and these cases open a new horizon in this matter. These cases are paramount in clinical practice and the safety and success rate of surgical procedures [18-21]. The instance reported by Hagemann et al. illustrates this point where an MN to MCN transfer was abandoned because of a neuroanatomical variation [22].
Conclusion
We report a case with several variations in the MN in its course and branching. Surgeons should be aware of these variations to maximize the success rate of surgical operations and ensure patient safety. Familiarity with the path of peripheral nerves is crucial for explaining sensory and motor loss during injuries and the occurrence of musculoskeletal diseases. In addition, it can aid in diagnostic methods such as electromyography (EMG).
Acknowledgments: The authors express their heartfelt appreciation to the individuals who willingly donated their bodies for the advancement of anatomical research. The findings from these studies can enhance medical treatment. Therefore, our sincere gratitude is due to these donors and their families.
Conflicts of interest and sources of funding: This study did not receive any dedicated funding from public, commercial, or not-for-profit organizations.
References
- Kumari A, Sinha BK. Study of Surgical Importance of Variations and Branching Pattern of Median Nerve at Carpal Tunnel. Eur J Mol Clin Med. 2021; 8(4): 2236-2243.
- Johnson E, Vekris M, Demesticha T. Neuroanatomy of the brachial plexus: normal and variant anatomy of its formation. Surg Radiol Anat. 2010; 32: 291-297.
- Williams PL, Warwick R, Dyson M, Bannister LH. Gray’s anatomy. 37th ed. London: Churchill Livingstone; 1989.
- Grant’s dissector. 14th ed. Lippincott, Williams & Wilkins; 2008.
- Romans J. Cunningham’s Manual of Practical Anatomy. Vol 2. 1998.
- Ferreira Arquez H. Anastomosis Between Ulnar And Radial Nerve: A Cadaveric Study. Int Arch Med. 2017; 10.
- Venieratos D, Anagnostopoulou S. Classification of communications between the musculocutaneous and median nerves. Clin Anat. 1998; 11(5): 327-331.
- Demircay E, Kabatas S, Cansever T, Yilmaz C. An anatomical variation of the third common digital nerve and recurrent motor branch of the median nerve. Neurol India. 2009 May-Jun; 57(3): 337-9. doi: 10.4103/0028-3886.53281. PMID: 19587480.
- Mat Taib C, Hassan S, Esa N, Mohd Moklas M, San A. Anatomical variations of median nerve formation, distribution and possible communication with other nerves in preserved human cadavers. Folia Morphol. 2017; 76(1): 38-43.
- Ballesteros LE, Forero PL, Buitrago ER. Communication between the musculocutaneous and median nerves in the arm: an anatomical study and clinical implications. Rev Bras Ortop. 2014 Dec 27; 50(5): 567-572. doi: 10.1016/j.rboe.2014.08.009. PMID: 26535190; PMCID: PMC4610987.
- Spagnoli AM, Fino P, Fioramonti P, Sanese G, Scuderi N. Bifid median nerve and carpal tunnel syndrome: an uncommon anatomical variation. Ann Ital Chir. 2017; 88: 95-96.
- Amadio PC. Anatomic variations of the median nerve within the carpal tunnel. Clin Anat. 1988; 1(1): 23-31. doi: 10.1002/ca.980010106.
- Narayan S. Bifid median nerve in a patient with carpal tunnel syndrome: A case report and literature review. Australas J Ultrasound Med. 2016 Nov 21; 19(4): 164-168. doi: 10.1002/ajum.12029.
- Yerasu MR, Ali M, Rao R, Murthy JMK. Bifid median nerve: a notable anomaly in carpal tunnel syndrome. BMJ Case Rep. 2022 May 17; 15(5): e249220. doi: 10.1136/bcr-2022-249220. PMID: 35580937; PMCID: PMC9114938.
- Spagnoli AM, Fino P, Fioramonti P, Sanese G, Scuderi N. Bifid median nerve and carpal tunnel syndrome: an uncommon anatomical variation. Ann Ital Chir. 2017; 88: 95-96. PMID: 28447963.
- Lonie S, Niumsawatt V, Rozen WM. Median Nerve Trifurcation. Plast Reconstr Surg Glob Open. 2016 Nov 23; 4(11): e1129. doi: 10.1097/GOX.0000000000001129. PMID: 27975031; PMCID: PMC5142497.
- Stancić MF, Eskinja N, Stosić A. Anatomical variations of the median nerve in the carpal tunnel. Int Orthop. 1995; 19(1): 30-34.
- Hagemann C, Stücker R, Breyer S, et al. Nerve transfer from the median to musculocutaneous nerve to induce active elbow flexion in selected cases of arthrogryposis multiplex congenita. Microsurgery. 2019; 39(8): 710-714. doi: 10.1002/micr.30451.
- Isaacs J, Ugwu-Oju O. High median nerve injuries. Hand Clin. 2016; 32(3): 339-348. doi: 10.1016/j.hcl.2016.03.004.
- Kara AB, Elvan Ö, Öztürk NC, et al. Communications of the median nerve in foetuses. Folia Morphol. 2018; 77(3): 441-446. doi: 10.5603/FM.a2017.0107.
- Sunderland S. The anatomy and physiology of nerve injury. Muscle Nerve. 1990; 13(9): 771-784. doi: 10.1002/mus.880130903.
- Demircay E, Kabatas S, Cansever T, Yilmaz C. An anatomical variation of the third common digital nerve and recurrent motor branch of the median nerve. Neurol India. 2009 May-Jun; 57(3): 337-9. doi: 10.4103/0028-3886.53281. PMID: 19587480.