
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Jugular vein phlebectasia presenting as transient neck swelling on exertion: A case report
Sachin Bhatt1*; Sanjay Kumar2; Tapasya Bishnoi2; Marlapudi Sudheer kumar1; Angshuman Dutta3; Bhanu Pratap Singh4
1Resident, Department of ENT-HNS, Command Hospital Airforce, Bangalore, India.
2Associate Professor, Department of ENT-HNS, Command Hospital Airforce, Bangalore, India.
3Consultant & Head of Department of ENT-HNS, Command Hospital Airforce, Bangalore, India.
4Professor, Department of Radiodiagnosis, Command Hospital Airforce, Bangalore, India.
*Corresponding Author : Sachin Bhatt
Resident, Department of ENT-HNS, Command Hospital Airforce, Bangalore, India.
Tel: +91-7507316452;
Email: bhatt.sachin18@gmail.com
Received : Jun 04, 2024
Accepted : Jun 18, 2024
Published : Jun 25, 2024
Archived : www.jcimcr.org
Copyright : © Bhatt S (2024).
Abstract
Jugular vein phlebectasia represents a distinctive form of venous anomaly characterized by an aberrant, fusiform dilatation primarily involving the neck’s venous system, predominantly the Internal Jugular Vein (IJV) and, to a lesser extent, the External Jugular Veins (EJV). Accounting for approximately two-thirds of all cases, IJV phlebectasia manifests more frequently in males, presenting a benign course with most cases being asymptomatic. The condition is often identified incidentally, with the chief complaint typically related to cosmetic concerns. Clinically, it is characterized by a soft, round, or fusiform, painless, and compressible neck swelling, notably positioned at the lower third of the anterior border of the sternocleidomastoid muscle. This swelling exhibits a characteristic increase in size during activities that elevate intrathoracic pressure, such as straining, coughing, performing the Valsalva maneuver, or engaging in physical exertion. Doppler ultrasonography (USG) emerges as a pivotal diagnostic tool, offering a non-invasive means to confirm the diagnosis by visualizing the venous dilatation and assessing its dynamic changes with intrathoracic pressure variations. Management of jugular vein phlebectasia predominantly adopts a conservative approach, reserving surgical intervention for cases presenting with significant complications, such as thrombosis or potential rupture. This case report delineates the clinical journey of a paediatric patient with jugular vein phlebectasia, emphasizing the diagnostic challenges and management decisions integral to such cases.
Keywords: Fusiform neck swelling; Neck swelling; Jugular vein; Phlebectasia.
Citation: Bhatt S, Kumar S, Bishnoi T, kumar MS, Dutta A, et al. Jugular vein phlebectasia presenting as transient neck swelling on exertion: A case report. J Clin Images Med Case Rep. 2024; 5(6): 3138.
Introduction
Jugular vein phlebectasia, characterized by an unusual, fusiform dilatation, predominantly affects the neck’s venous structures, with the Internal Jugular Vein (IJV) being implicated in about two-thirds of cases. This benign condition exhibits a higher prevalence in males and is most identified in children and young adults. It presents as a compressible, soft swelling that notably enlarges during activities that elevate intrathoracic pressure, such as straining, the Valsalva Maneuver, sneezing, or coughing, typically manifesting unilaterally. The differential diagnosis for this presentation is broad, spanning conditions like laryngocele, cystic hygroma, branchial cyst, and superior mediastinal mass, necessitating a comprehensive clinical evaluation for accurate diagnosis [1,2].
Given its rarity, jugular vein phlebectasia requires heightened clinical awareness and suspicion amongst healthcare providers for timely and accurate identification. The literature highlights the role of non-invasive imaging modalities, especially Doppler ultrasonography, in confirming the diagnosis due to its effectiveness and safety [3]. This case report not only sheds light on jugular vein phlebectasia as a significant, albeit rare, differential diagnosis for transient neck swelling but also highlights the diagnostic challenges and management decisions integral to such cases. Through the detailed presentation of a paediatric patient, this report aims to contribute uniquely to the existing body of knowledge, highlighting the importance of a meticulous approach to diagnosis and management in young patients with this condition, thereby encouraging a proactive diagnostic and therapeutic approach among clinicians.
Case summary
A four-year-old male was brought to medical attention by his parents, who were concerned about a persistent right-sided neck swelling that had gradually enlarged over a period of six months. The swelling notably increased during activities that elevated intrathoracic pressure, such as coughing or straining (Figures 1a & 1b). No fever, pain, history of trauma, cough, weight loss, or difficulties in swallowing and breathing were associated with this swelling. Furthermore, no additional swellings were detected elsewhere on the patient’s body.
Upon physical examination, a 2 cm x 2 cm, non-pulsatile, non-tender, and non-transilluminating swelling was identified on the right side of the neck. This swelling displayed a compressible, cystic nature and transiently increased in size during continuous speech (Figures 1a & 1b). Importantly, there was no pulsation or bruit over the swelling area, and no other neck swellings or cervical lymphadenopathy were observed.
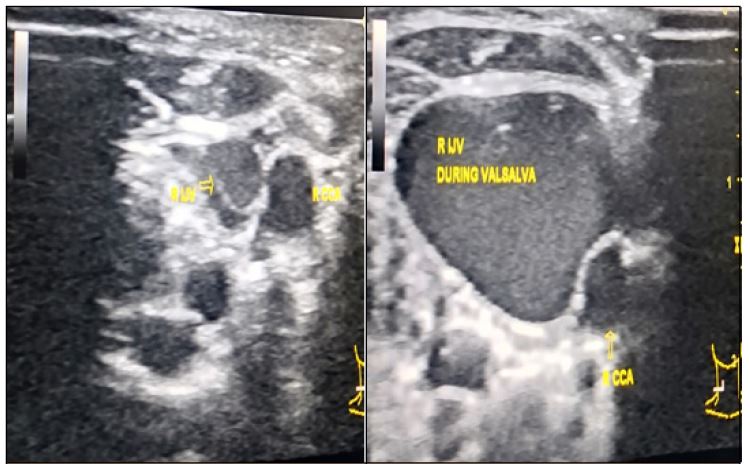
Diagnostic imaging played a crucial role in the evaluation of this case. A lateral neck X-ray, initially performed, revealed no abnormalities, directing the diagnostic focus towards more specialized imaging techniques. Ultrasonography of the neck proved instrumental in identifying the condition, revealing a diagnosis of right internal jugular vein phlebectasia. Measurements taken during the ultrasonography showed a pre-Valsalva diameter of the internal jugular vein at 7.9 mm, which increased to 11.1 mm post-Valsalva (Figures 2a,b). These findings indicated a significant dilatation upon increased intrathoracic pressure. The diagnosis was further supported by normal findings in both a chest X-ray and 2D echocardiography, conducted to exclude any associated cardiac anomalies.
Given the asymptomatic nature of the condition and after a comprehensive review of the child’s diagnosis, a conservative management approach was adopted, aligning with current best practices for managing jugular vein phlebectasia in pediatric patients. The parents were provided reassurance about the benign nature of the condition and advised on the importance of regular follow-up visits. These visits were intended to monitor any changes in the swelling’s size or the emergence of new symptoms. The patient has been under semi-annual surveillance for one year, during which no complications or progression of the condition have been observed.
Throughout the follow-up period, careful observation was maintained to assess any potential changes in the swelling’s characteristics or any new symptoms that might indicate a shift in the condition’s trajectory. These follow-up visits also served as educational opportunities for the parents, emphasizing the importance of recognizing signs that could warrant immediate medical attention. This proactive approach not only ensured the patient’s continued well-being but also empowered the caregivers with knowledge and reassurance.
This case highlights the crucial role of detailed clinical examination and targeted diagnostic imaging in identifying jugular vein phlebectasia. Through vigilant monitoring and a conservative management strategy, a stable course was observed without the need for invasive interventions, highlighting the efficacy of such an approach in managing selected cases of this rare venous anomaly.

Discussion
Jugular vein phlebectasia, defined as a non-tortuous dilatation of a vein, is a distinguished clinical entity within the spectrum of vascular anomalies. First described by Zukschwerdt in 1929 [4], it has been variously termed venous ectasia, congenital venous cyst, venous aneurysm, or essential venous dilatation, reflecting its diverse presentations and underlying mechanisms. Although it may affect any vein, the Internal Jugular Veins (IJVs), followed by External Jugular Veins (EJVs), are most commonly involved, with less frequent involvement of anterior jugular and superficial communicans veins. This prevalence in the IJV was also evident in the case under discussion, reinforcing the condition’s characteristic patterns.
The clinical manifestation of jugular vein phlebectasia is often benign and asymptomatic, predominantly affecting males and typically presenting as a cosmetic concern. This aligns with existing literature that highlights the condition’s hallmark features: a soft, compressible neck swelling that exacerbates with manoeuvres elevating intrathoracic pressure [5]. The case presented herein validates these observations, particularly noting the swelling’s transient enlargement with exertion, serving as a crucial diagnostic indicator.
Etiological hypotheses and differential diagnosis
Etiological hypotheses for jugular vein phlebectasia incorporate congenital factors such as a primary deficiency in venous wall elasticity, elevated venous pressure, and anatomical considerations like the proximity of the right innominate vein to the right apical pleura, potentially explaining the condition’s right-side predilection [6]. The multifactorial aetiology suggested by these hypotheses mirrors the complexities observed in the discussed case, indicating a need for further exploration.
The differential diagnosis for jugular vein phlebectasia is broad, including conditions like laryngocele, pulmonary apical bullae, and superior mediastinal cysts. This highlights the necessity for a detailed diagnostic approach. In the case reviewed, Doppler ultrasonography was pivotal, echoing literature advocating its utility in the non-invasive, real-time assessment of the vein’s morphology and hemodynamic [7].
Management strategies
The management of jugular vein phlebectasia generally involves observation and follow-up, with surgical intervention considered for cases with complications or significant cosmetic concerns [8]. This conservative approach, mirrored in the case management strategy, reflects the condition’s benign nature and the rarity of complications such as thrombosis and Horner’s syndrome.
Future directions
Despite the infrequency of spontaneous rupture, the literature discusses surgical options ranging from IJV ligation to more complex procedures like longitudinal constriction suture venoplasty, indicating the necessity for tailored management plans. Furthermore, the potential role of prophylactic anticoagulants in preventing thrombosis in these patients highlights an area for research, suggesting that understanding of jugular vein phlebectasia continues to evolve [8].
Conclusion
This case study highlights the critical importance of accurately identifying jugular vein phlebectasia and comprehending its implications for patient care. It has been demonstrated that, although a conservative management strategy is typically preferred, medical professionals must maintain vigilance and be prepared to explore surgical interventions should complications present themselves. Through diligent monitoring and the implementation of a treatment plan that is customized to the patient’s specific needs, optimal patient outcomes can be achieved. This approach not only exemplifies the significance of informed clinical decision-making in the management of jugular vein phlebectasia but also highlights the necessity for healthcare providers to adapt their strategies based on the evolving clinical presentation of the condition.
Compliance with ethical standards
No conflicts of interest.
No research involving human participants or animals was conducted.
Informed/written consent was taken from the parents of the child for the publication of the case study.
No funding was provided for the creation of this manuscript.
There are no material financial or non-financial interests to disclose by the authors.
References
- Afzal M, Mohamed AH, Volkin Y. It’s a bird! it’s a plane! it’s a vein! jugular vein phlebectasia in a pediatric patient with tracheomalacia. Cureus [Internet]. 2023 Jul 31; Available from: https://doi.org/10.7759/cureus.42746
- Singh H, Maurya V, Satua L, Saini MK. Internal Jugular Phlebectasia. Medical Journal Armed Forces India [Internet]. 2001; 57(1): 70-1. Available from: https://doi.org/10.1016/s0377-1237(01)80100-3
- Uzun C, Taşkınalp O, Koten M, Adalı MK, Karasalihoğlu A, Pekindil G. Phlebectasia of left anterior jugular vein. The Journal of Laryngology & Otology [Internet]. 1999; 113(9): 858–60. Available from: https://doi.org/10.1017/s0022215100145426
- Kesarwani A, Goyal A, Kumar A. Phlebectasia of Internal Jugular Vein- A Rare Differential Case of Neck Swelling with Review of Literature. Iran J Otorhinolaryngol. 2019; 31(105): 239-242. PMID: 31384591; PMCID: PMC6666941.
- Bindal SK, Vasisth G, Chibber P. Phlebectasia of internal jugular vein. Journal of Surgical Technique and Case Report [Internet]. 2012; 4(2): 103. Available from: https://doi.org/10.4103/2006-8808.110266
- Li J, Jiang X, Hu T. Surgical treatment of jugular vein phlebectasia in children. The American Journal of Surgery [Internet]. 2006; 192(3): 286–90. Available from: https://doi.org/10.1016/j.amjsurg.2006.02.025
- Yokomori K, Kubo K, Kanamori Y, Takemura T, Yamamoto T. Internal jugular phlebectasia in two siblings: Manometric and histopathologic studies of the pathogenesis. Journal of Pediatric Surgery [Internet]. 1990; 25(7): 762–5. Available from: https://doi.org/10.1016/s0022-3468(05)80014-4
- Hu X, Li J, Hu T, Jiang X. Congenital jugular vein phlebectasia. American Journal of Otolaryngology [Internet]. 2005; 26(3): 172–4. Available from: https://doi.org/10.1016/j.amjoto.2005.02.009