
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Radio-clinical histologic diagnosis of huge rhino-orbito-cerebral mycotic mass
Emmanuel Garba Sunday1; Nasiru Raheem2; Eno-Abasi Garba Sunday3*; Aminu Saad Jika2; Daniel Vahyella4; Yao Christian Hugues Dokponou5
1Department of Surgery, Neurosurgery Unit, Modibbo Adama University Teaching Hospital, Yola, Adamawa State, Nigeria.
2Department of Anatomic Pathology and Forensic Medicine, Modibbo Adama University Teaching Hospital, Yola, Adamawa State, Nigeria.
3Department of Paediatrics, Haematology and Oncology Unit, University of Ilorin Teaching Hospital, Ilorin, Kwara State, Nigeria.
4Department of Surgery, Modibbo Adama University Teaching Hospital, Yola, Adamawa State, Nigeria.
5Department of Neurosurgery, Mohammed V University of Medicine and Pharmacy of Rabat, Morocco.
*Corresponding Author : Emmanuel G Sunday
Department of Surgery, Neurosurgery Unit, Modibbo Adama University Teaching Hospital, Yola, Adamawa State, Nigeria.
Email: emistocrate@yahoo.com
Received : Jun 04, 2024
Accepted : Jun 18, 2024
Published : Jun 25, 2024
Archived : www.jcimcr.org
Copyright : © Sunday EG (2024).
Keywords: Mycotic mass; Intracranial; Orbit; Sinuses; Clinical; Radiology; Histopathology.
Citation: Sunday EG, Raheem N, Sunday EG, Jika AS, Vahyella D, et al. Radio-clinical histologic diagnosis of huge rhino-orbito-cerebral mycotic mass. J Clin Images Med Case Rep. 2024; 5(6): 3139.
Description
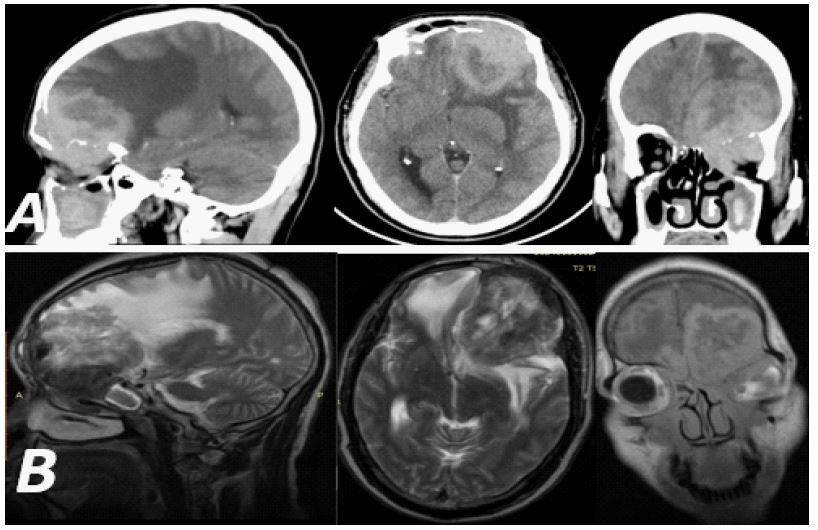
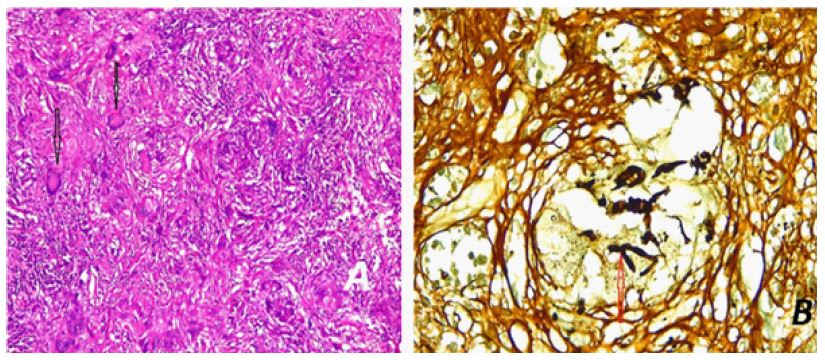
We present a difficult diagnosis of an unusual intracranial fungal mass in a male farmer aged 50 years who is immunocompetent and right-handed. His cranial CT scan showed a left mass extending into the sphenoid sinus, with a necrotic core and calcifications. The lesion eroded the orbital roof and invaded the left maxillary sinus (Figure 1a). He had been seen for about a year by a general practitioner, a psychiatrist, and a neurologist, in that order, for behavioural changes, frontal headache, right spastic hemiparesis, and left proptosis. For this reason, he was referred to our facility. His schizophrenia was treated and when neurological symptoms appeared, he was referred to neurology. Aside from the fact that he was a farmer and may have been exposed to the infectious organism through plants or soil, his medical history was unremarkable. Brain MRI results at presentation showed a massive left rhino-orbito-sub frontal mass of mixed intensity that destroyed the orbital roof and invaded the frontal lobe, displacing it superiorly and extending into the left maxillary sinus and sphenoid sinus (Figure 1b). We considered the clinical differentials of fibrous dysplasia and left sub frontal atypical meningioma. The patient underwent total resection of a severely fibrous tumour, recovered well from surgery, was able to walk on the first postoperative day, and tolerated oral drug administration. However, on the fourth postoperative day, he developed a fever with leucocytosis and neutrophilia, and the site of infection could not be identified. He was given empirical triple antibiotics, but he did not respond and died on the 8th postoperative day. The histological result was available the next day, and revealed chronic granulomatous inflammation, with epithelioid cells, fibrosis, and multinucleated giant cells (Figure 2a), suggesting rhinoorbitocerebral mycoses, most likely due to aspergillosis (Figure 2b).
Hippocrates was the first to describe candidiasis. In 1861, Zenker [4] was the first to describe intracerebral candidiasis in a dead patient. In 1897, Oppe was the first to describe rhino-orbito-cerebral aspergillosis while Gregory described detailed cases of rhino-orbito-cerebral zygomycosis [4]. Fungal infections of the Central Nervous System (CNS) are rare diseases (only about 10-15% of identified fungi lead to systemic or CNS infection) [4], even in large agricultural societies such as India [1], are usually associated with diagnostic difficulties in the presence of immunosuppression or direct inoculation after cranial neurosurgical procedures. CNS fungal infections can cause various syndromes such as hydrocephalus, basal meningitis, and space-occupying lesions such as granulomas and brain abscesses. Although rare, it results in high morbidity and mortality compared to other CNS infections (bacterial, viral, parasitic) [1-4]. Therefore, the strategy for a good outcome is early detection and prompt initiation of surgical and medical therapy (organism-based, with triazoles (voriconazole) and echinocandins being the newest effective drugs) [1,4].Hippocrates was the first to describe candidiasis. In 1861, Zenker [4] was the first to describe intracerebral candidiasis in a dead patient. In 1897, Oppe was the first to describe rhino-orbito-cerebral aspergillosis while Gregory described detailed cases of rhino-orbito-cerebral zygomycosis [4]. Fungal infections of the Central Nervous System (CNS) are rare diseases (only about 10-15% of identified fungi lead to systemic or CNS infection) [4], even in large agricultural societies such as India [1], are usually associated with diagnostic difficulties in the presence of immunosuppression or direct inoculation after cranial neurosurgical procedures. CNS fungal infections can cause various syndromes such as hydrocephalus, basal meningitis, and space-occupying lesions such as granulomas and brain abscesses. Although rare, it results in high morbidity and mortality compared to other CNS infections (bacterial, viral, parasitic) [1-4]. Therefore, the strategy for a good outcome is early detection and prompt initiation of surgical and medical therapy (organism-based, with triazoles (voriconazole) and echinocandins being the newest effective drugs) [1,4].
References
- Gandhi A, Jain S, Gandhi S, Mishra K, Jain SK. Intracranial Mass Lesion Due to Fungal Infection: A Case Series and Review of Literature. Iranian Journal of Neurosurgery. 2020; 6(3): 143-50.
- Rajshekhar V, Rajshekhar V. Surgical management of intracranial fungal masses. Neurology India. 55.
- Mishra A, Prabhuraj AR, Shukla DP, Nandeesh BN, Chandrashekar N, Ramalingaiah A, et al. Intracranial fungal granuloma: A single-institute study of 90 cases over 18 years. Neurosurg Focus. 2019; 47(2).
- Raman Sharma R. Fungal infections of the nervous system: Current perspective and controversies in management. International Journal of Surgery. 2010; 8: 591-601.