
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A case of neuroendocrine tumor misdiagnosed as autoimmune pancreatitis
Yue Liu; Chang Wu; Donglin Wan; Deyu Zhang; Haojie Huang*
Department of Gastroenterology, Changhai Hospital, Second/Navy Military Medical University, Shanghai, China.
*Corresponding Author : Haojie Huang
Department of Gastroenterology, Changhai Hospital, Second/Navy Military Medical University, Shanghai, China.
Email: huanghaojie@smmu.edu.cn
Received : May 29, 2024
Accepted : Jun 20, 2024
Published : Jun 27, 2024
Archived : www.jcimcr.org
Copyright : © Huang H (2024).
Citation: Liu Y, Wu C, Wan D, Zhang D, Huang H. A case of neuroendocrine tumor misdiagnosed as autoimmune pancreatitis. J Clin Images Med Case Rep. 2024; 5(6): 3142.
Case report
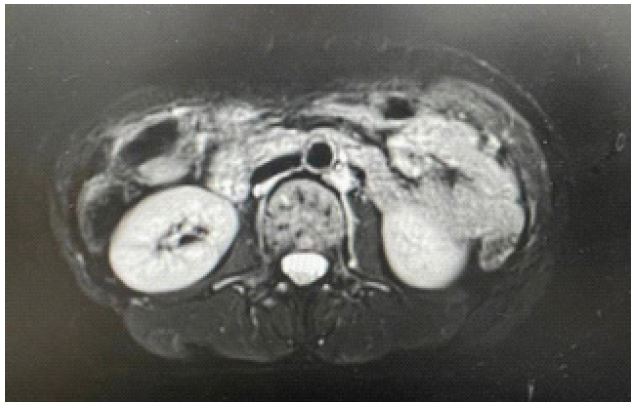
A 47-year-old woman presented with recurrent abdominal distension for more than 2 years. The patient developed a feeling of fullness in the upper and middle abdomen after eating food 2 years ago. There was no nausea, vomiting, abdominal pain, diarrhea, acid regurgitation or heartburn. Gastroscopy in another hospital showed chronic superficial gastritis with erosion and biliary reflux. After taking omeprazole and other acid suppressants for a period of time, the symptoms disappeared and the medication was stopped. Gastroscopy in the other hospital showed chronic superficial gastritis with erosion, and abdominal distension was not significantly relieved after taking acid suppressants. On June 17, 2023, contrast-enhanced CT in the middle and upper abdomen showed diffuse enlargement of the pancreas with uneven enhancement, and malignant tumor. Autoimmune pancreatitis? On June 28, 2023, he was admitted to the outpatient department of Gastroenterology of our hospital, and his immunoglobulin G4 (IgG4) was 1.25g/L. Blood routine test showed eosinophil count 0×109 /L, eosinophil percentage 0%. Liver function tests showed AST mitochondrial isoenzyme 3.1U/L, γ -glutamyl transpeptidase 113 U/L, alkaline phosphatase 115U/L, and aspartate aminotransferase 14 U/L. Hemoglobin A1c 9.6%; Tumor markers: carcinoembryonic antigen 3.24 ng/ml, carbohydrate antigen 199 8.85 U/ml. Physical examination: flat abdomen, no abdominal muscle tension, no tenderness, rebound pain. The liver and spleen were not palpable, and the family history was normal. Blood routine test showed eosinophil 0.03×109 /L and percentage of eosinophil 0.7%. On July 8, 2023, pancreas enhanced MRI showed pancreatic swelling, heterogeneous pancreatic signal, pancreatic changes, consistent with autoimmune pancreatitis, and pancreatic duct dilatation. After painless endoscopic ultrasonography, diffuse enlargement of the gland was found, and a round hypoechoic lesion was seen in the body and tail of the pancreas. The maximum section was about 4.5x2.9 cm, and the hypoechoic pancreatic mass was found. EUS-FNA; Puncture pathology: cytology smear: (pancreatic puncture) no malignant cells were found; Liquid-based cytology showed tumor cells were found, epithelial origin, mild atypia, consistent with neuroendocrine tumors. Immunohistochemical: CAM5.2 (+), CK7 (-), CgA (+), Syn (+), CD56 (+), INSMI (+), ATRX (+), RB (+), CD38 (-), SSTR2 (+), p53 (< 5%), Ki67 (2%). Combined with immunohistochemical staining results, (pancreatic puncture) neuroendocrine tumor was considered as NET-G1 grade. Blood routine test on July 17, 2023: eosinophil 0×109 /L, eosinophil percentage 0%; Autoimmune antibodies were negative. Tumor markers: Alpha-fetoprotein (AFP) 2.48 ng/ml, carcinoembryonic antigen 3.4 ng/ml, carbohydrate antigen CA199 10.09 U/ml. On July 22,2023, the patient was admitted to the Department of Pancreatic surgery for suspected “pancreatic tumor”. On July 20,2023, pancreatic artery CT enhancement was considered to indicate pancreatic sausage like swelling and pancreatic changes. Consistent with the manifestations of autoimmune pancreatitis, total pancreatectomy + splenectomy + portal vein lateral wall resection and reconstruction + retroperitoneal lymph node dissection under general anesthesia was performed on July 25, 2023. During the operation, a mass with a maximum diameter of >3 cm was palpable in the head, neck and body of the pancreas, the surface was not smooth, the boundary was unclear, and the activity was acceptable, with nerve involvement. Suspected lymph node metastasis was observed around the mass. Postoperative https://fanyi.youdao.com/download pathology showed total pancreatic neuroendocrine tumor (NET G2), and the tumor partially grew along the main pancreatic duct and branch pancreatic duct. On September 14, 2023, the enhanced MRI of the pancreas showed postoperative changes of the pancreas, multiple metastatic tumors in the liver, and scattered diffuse limited slightly large lymph nodes near the mesenteric vessels. Radiofrequency ablation was performed in the Hongkou branch of our hospital on October 28, 2023.

Discussion
pancreatic neuroendocrine neoplasm (pNEN) is a relatively rare tumor, but the incidence of PNEN has increased in recent years [1]. pNEN can be divided into functional and nonfunctional categories according to whether the patient has the corresponding clinical manifestations due to the secretion of hormones by the tumor. Functional pNEN accounted for 34.4% and non-functional pNEN accounted for 65.6% [2]. The most common primary sites of neuroendocrine tumors in China are pancreas, rectum and stomach [3]. Due to its onset in the pancreas, its clinical manifestations are insidious and its biological characteristics are highly heterogeneous, which makes its diagnosis and treatment difficult. In clinical practice, serum chromogranin A (CgA) and neuron specific enolase (NSE) are often used to assist in the diagnosis and determination of tumor burden, and even to evaluate the efficacy and prognosis [4]. In addition, the levels of hormones, such as gastrin, insulin, glucagon, etc., can also be detected to determine the type and whether the tumor is functional. In terms of imaging evaluation, CT or MRI methods are often used for localization diagnosis and clinical staging of non-functional pNEN. The sensitivity and specificity of spectral CT combined with perfusion in the diagnosis of neuroendocrine tumors were 83.1%-96.2% [5], and MRI was superiorto CT in the diagnosis of liver metastases and small pancreatic lesions [6]. Compared with MRI and CT, the overall sensitivity and specificity of EUS in the diagnosis of pancreatic neuroendocrine tumors were 86.0% and 89.7% respectively [7]. The gold standard for the diagnosis of non-functional pNEN is pathology. Eus can directly obtain histopathological specimens through fine needle aspiration, which is conducive to the localization and qualitative diagnosis of non-functional pNEN. In terms of treatment, surgical resection is an important treatment for nonfunctional pNEN [8], and surgical resection is the main treatment for local tumors. The liver is the most common distant metastasis site of nonfunctional pNEN. The main treatment options for liver metastases include radiofrequency ablation, transcatheter arterial embolization, and transcatheter arterial chemoembolization [9]. When the primary lesion cannot be completely resected or combined with surgical risk factors, medical treatment can be selected, such as immune checkpoint inhibitors (pembrolizumab, etc.), biological therapy (octreotide, etc.), targeted drugs (sunitinib, etc.), radionuclide scanning, etc. to delay the survival times of patients [10]. When the tumor involves the whole pancreas, it needs to be differentiated from autoimmune pancreatitis and other diseases. Autoimmune pancreatitis (AIP) is a special type of chronic pancreatitis, which is characterized by local or diffuse enlargement of the pancreas, irregular narrowing of the main pancreatic duct, elevated serum immunoglobulin G4 (IgG4), accumulation of other organs, and steroid therapy [11]. According to its morphology, autoimmune pancreatitis can be divided into diffuse type and focal type on imaging [12]. Although AIP usually shows diffuse enlargement of the pancreas with a saussure-like appearance, delayed enhancement and band-like structure, and capsule formation on imaging findings [13], it still needs to be differentiated from other diseases. In order to avoid misdiagnosis and delay surgery, it is necessary to distinguish diffuse AIP from pancreatic neuroendocrine tumors [14]. Although it is rare in clinic, it still needs to be paid attention to by clinicians. The patient was a middle-aged woman with a long course of disease, 2 years of nonspecific abdominal distension and imaging findings similar to AIP. Endoscopic ultrasound guided fine needle aspiration (EUS-FNA) was performed to obtain pancreatic tissue for pathological examination, and the final diagnosis was non-functional pNEN. Total pancreatectomy was performed. Therefore, it is very important to differentiate non-functional pNEN from AIP. We suggest that when the clinical features are nonspecific, the imaging diagnosis is unclear, and the IgG4 level is not increased, EUS-guided fine needle aspiration biopsy should be performed to confirm the pathological diagnosis.
References
- Zhang X, Ma L, Bao H, et al. Clinical, pathological and prognostic characteristics of gastroenteropancreatic neuroendocrine neoplasms in China: a retrospective study. BMC Endocr Disord. 2014; 14: 54.
- Wu W, Jin G, Li H, et al. The current surgical treatment of pancreatic neuroendocrine neoplasms in China: a national wide cross-sectional study. Journal of Pancreatology. 2019; 2.
- Song L, Zhai X, Yu S, et al. Clinical analysis of 547 patients with neuroendocrine tumors in a Chinese population: A single-center study. Cancer Med. 2019; 8: 3729-3737.
- Yang X, Yang Y, Li Z, et al. Diagnostic value of circulating chromogranin a for neuroendocrine tumors: a systematic review and meta-analysis. PLoS One. 2015; 10: 0124884.
- Li Z, Chen Y, Zhang Y, et al. Quantitative energy spectrum CT in differential diagnosis of aldosterone-producing adenoma and cortisol-producing adenoma. Quant Imaging Med Surg. 2023; 13: 5012-5021.
- Xu Tianming Li. Progress in diagnosis and treatment of pancreatic neuroendocrine tumors. Journal of Clinical Internal Medicine 2023; 40(09): 581-3.
- Chen Y, Huang F, Fan Y, et al. Diagnostic value of endoscopic ultrasound for detecting pancreatic neuroendocrine tumors: A systematic review and meta-analysis. Am J Med Sci. 2022; 363: 511-518.
- Vaghaiwalla T, Keutgen XM. Surgical Management of Pancreatic Neuroendocrine Tumors. Surg Oncol Clin N Am. 2020; 29: 243-252.
- Hain E, Sindayigaya R, Fawaz J, et al. Surgical management of pancreatic neuroendocrine tumors: an introduction. Expert Rev Anticancer Ther. 2019; 19: 1089-1100.
- Liang Yun Wu, Nie Yongzhan, Chen Jie. Interpretation of “Chinese Anti-Cancer Association Guidelines for the Diagnosis and Treatment of Neuroendocrine Tumors (2022 Edition)”. Journal of Peking Union Medical College 2023;14(01):94-100.
- Okazaki K, Kawa S, Kamisawa T, et al. Amendment of the Japanese consensus guidelines for autoimmune pancreatitis. 2020. J Gastroenterol. 2022; 57: 225-245.
- Frulloni L, Scattolini C, Falconi M, et al. Autoimmune pancreatitis: differences between the focal and diffuse forms in 87 patients. Am J Gastroenterol. 2009; 104: 2288-94.
- Irie H, Honda H, Baba S, et al. Autoimmune pancreatitis: CT and MR characteristics. AJR Am J Roentgenol. 1998; 170: 1323-7.
- Onda S, Okamoto T, Kanehira M, et al. Histopathologically proven autoimmune pancreatitis mimicking neuroendocrine tumor or pancreatic cancer. Case Rep Gastroenterol. 2012; 6: 40-6.