
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Rare cause of pneumothorax: Birt Hogg Dube syndrome
*Corresponding Author : Caner Çinar
Department of Internal Medicine, Division of Oncology, Marmara University Medical Faculty, Istanbul, Turkey.
Email: dr.canercinar@gmail.com
Received : Jun 02, 2024
Accepted : Jun 21, 2024
Published : Jun 28, 2024
Archived : www.jcimcr.org
Copyright : © Çinar C (2024).
Citation: Çinar C. Rare cause of pneumothorax: Birt Hogg Dube syndrome. J Clin Images Med Case Rep. 2024; 5(6): 3145.
Introduction
Birt Hogg Dube Syndrome (BHDS) is an autosomal dominant inherited disease described in 1977. It is characterized by benign skin hamartomas often located on the head and neck, lung cysts, spontaneous pneumothorax and increased risk of kidney cancer. It is seen that the FLCN gene mutation encoding the structural follicle protein in BHDS. Although the exact incidence is not known, approximately 600 families have been identified worldwide [1]. The syndrome is likely to be underdiagnosed as it is thought that there may be more families with BHDS [2]. It has been reported that the follicle protein, whose structure is disrupted by multiple mutations, may have a tumor suppressor role, and therefore, kidney cancer, which is the most serious complication of the syndrome, should be followed closely [3]. In this case, a 47-year-old female patient diagnosed with BHDS is presented [4].
Case presentation
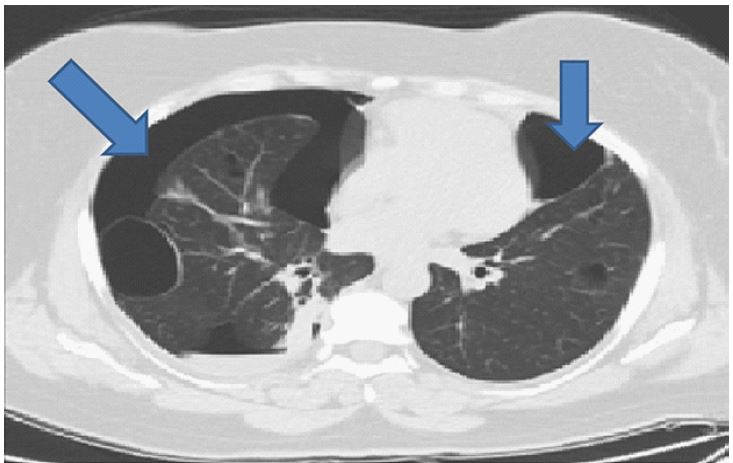
The patient’s pneumothorax history starts 3 years ago; it was learned that tube thoracostomy was performed due to the diagnosis of spontaneous pneumothorax in the center where the patient applied with the complaint of acute onset of chest pain, which woke her up at night. The same clinical picture recurred approximately 9 months later after first episode, second pneumothorax of the patient can be seen in Figure 1.
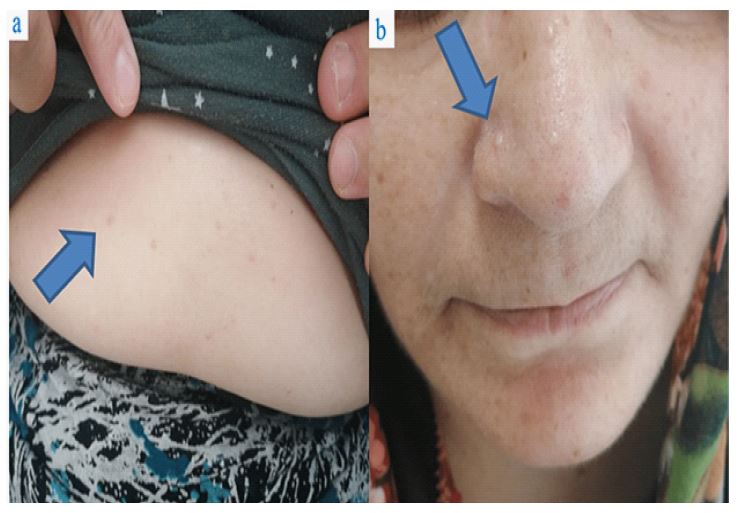
Then, right bullectomy was performed with video-assisted thoracoscopic surgery, and in the pathological tissue evaluation, she was diagnosed with bulla, bleb, emphysema and fibrinous pleuritis. The patient, who did not have a history of smoking and no other risk factors for developing cystic lung lesions, was consulted on the grounds that she had bilateral peripheral diffuse cystic lesions in the lung. On physical examination multiple millimetric skin-colored papules on the nose and epigastric skin was observed as shown in Figures 2A-2B.
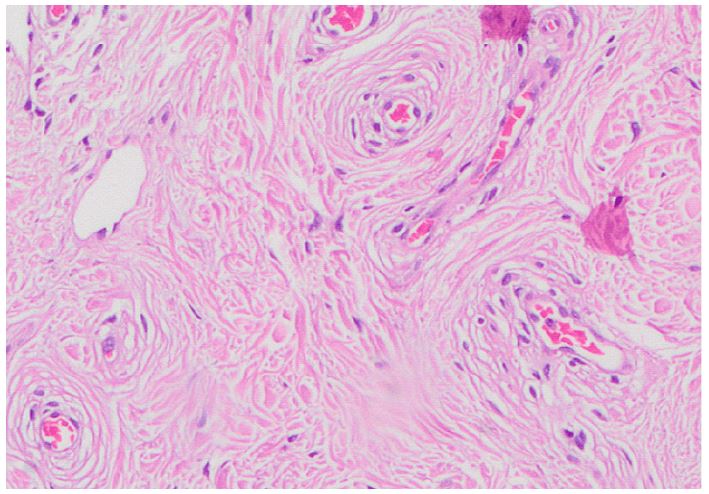
Punch biopsy to the lesions performed and pathological examination yielded data consistent with the trichodiscoma/fibrofolliculoma spectrum as we can see concentric fibrosis in Figure 3.
With all these data, the patient was diagnosed with Birt Hogg Dube Syndrome. This diagnosis was confirmed by the detection of similar lesions in the brother of the patient whose family was screened, and the biopsy results supported by BHDS. In the follow-up of the patient who had no respiratory complaints for two years, more prominent areas of suspicious pneumothorax were observed on the right, and a third tube thoracostomy was performed after healing she discharged from hospital and the outpatient follow-up of the patient continues.
Discussion
As described in our case BHDS is a rare syndrome worldwide, it is generally diagnosed late, and some patients continue their lives being undiagnosed. Appearance of pneumothorax due to air bulla should be a warning sign. Although both skin lesions and bullae were present in the first pneumothorax attack in this patient, it is seen that the diagnostic algorithm for BHDS has not progressed sufficiently. For these reasons, we recommend that detailed skin examinations of patients with bullae and pneumothorax be performed carefully. In this case, Lymphangioleiomyomatosis (LAM) or tuberosclerosis were excluded because cysts were not typically profuse and evenly distributed throughout both lungs as expected in LAM [5], pulmonary langerhans cell histiocytosis was excluded because there was a smoking history, and lymphoid interstitial pneumonia was excluded because there was no accompanying ground glass areas or autoimmune picture [6]. This patient was diagnosed with BHDS by meeting one of the two major diagnostic criteria, with the biopsy sample taken from multiple papular lesions on the skin of the nose and epigastric region reported as compatible with trichodiscoma/fibrodiscoma [7].
Demonstration of FLCN gene mutation, which is another major diagnostic criteria [8], comes to the fore in patients who have not yet had skin lesions. Studies have reported that the FLCN gene, which is involved in the pathophysiology of BHDS, has a tumor suppressor feature. Mutation of the gene results in BHDS, increasing the probability of renal cancer. There is not enough data in the literature on the formation of bullae in the lung with the mutation of the related gene. Further studies are needed to prove a possible relationship between FLCN gene mutation and multiple pulmonary bullae.
Conclusion
Birt-Hogg-Dubé Syndrome (BHDS) is rare autosomal dominantly inherited and generally underdiagnosed syndrome due to its varied clinical manifestations. BHDS should be considered in differential diagnoses of patients who presents with cystic lung lesion, recurrent pneumothorax history and skin lesions together. Early diagnosis is important in order to subject patients to systematic screening for possible underlying renal cancers. Lifelong surveillance for renal cancer is needed for patients who diagnosed with BHD syndrome.
References
- Lim DH, Rehal PK, Nahorski MS: A new locus-specific database (LSDB) for mutations in the folliculin (FLCN) gene. Hum Mutat. 2010; 31: 1043-1051. 10.1002/humu.21130.
- (2201619). https://bhdsyndrome.org/for-researchers/bhd-literature/introduction/published-bhd-families/.
- Eur Clin Respir J: Birt-Hogg-Dubé syndrome: a case report and a review of the literature. 2017; 10: 1080/20018525. 10.1080/20018525.2017.1292378.
- Toro J: Birt-Hogg-Dubé syndrome. 2014; 7: 1522-1993. 10.1001/archderm.135.10.1195.
- Tobino K, Gunji Y, Kurihara M, et al.: Characteristics of pulmonary cysts in Birt-Hogg-Dubé syndrome: thin-section CT findings of the chest in 12 patients. Eur J Radiol. 2011; 77: 403. 10.1016/j.ejrad.2009.09.004.
- Elia D, Torre O, Cassandro R, et al.: Pulmonary Langerhans cell histiocytosis: a comprehensive analysis of 40 patients and literature review. Eur J Intern Med. 2015; 26: 351. 10.1016/j.ejim.2015.04.001.
- Cha SI, Fessler MB, Cool CD, et al.: Lymphoid interstitial pneumonia: clinical features, associations and prognosis. Eur Respir J. 2006; 28: 364. 10.1183/09031936.06.00076705.
- Menko FH, van Steensel MA, Giraud S, Friis Hansen L, Richard S, Ungari S, Nordenskjöld M, Hansen TV, Solly J, Maher ER, European BHD. Consortium. 2009; 8: 1199-206. 10.1016/S1470-2045(09)70188-3.