
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Atypical presentation of sporotrichosis in an elderly patient
Júnia Marielle Teixeira Rodrigues Neri1*; Daniel Silva Junior1; Beatriz Bezerra De Oliveira1; Caroline Heleno Chagas De Carvalho2; Walter Belda Junior3
1Dermatologist, School of Medicine, University of São Paulo, Brazil.
2Volunteer Professor, Department of Dermatology, School of Medicine, University of São Paulo, Brazil.
3Associate Professor with Habilitation, Department of Dermatology, School of Medicine, University of São Paulo, Brazil.
*Corresponding Author : Júnia Marielle Teixeira Rodrigues Neri
Dermatologist, School of Medicine, University of São Paulo, Brazil.
Tel: +55-11-2661-3361 & +55-31-999844265;
Email: walterbelda26@gmail.com
Received : Jun 09, 2024
Accepted : Jun 24, 2024
Published : Jul 01, 2024
Archived : www.jcimcr.org
Copyright : © Rodrigues Neri JMT (2024).
Abstract
Sporotrichosis is a subacute or chronic mycosis caused by a thermodimorphic fungus of the genus Sporothrix. It is considered a cosmopolitan disease, mainly in tropical and subtropical regions, and is endemic in Latin America. In Brazil, there are two modes of transmission to humans: traumatic inoculation with contaminated soil and organic matter and zoonotic transmission (infected felines). In the present report, we present a case of sporotrichosis with an uncommon clinical presentation, located in a photo-exposed area of an elderly individual with actinic skin, and its excellent response to treatment with oral potassium iodide.
Keywords: Sporotrichosis; Potassium iodide; Treatment; Dermatology; Fungus.
Citation: Rodrigues Neri JMT, Junior DS, Oliveira BBD, Carvalho CHCD, Junior WB. Atypical presentation of sporotrichosis in an elderly patient. J Clin Images Med Case Rep. 2024; 5(7): 3146.
Introduction
Sporotrichosis is a subacute or chronic mycosis caused by a thermodimorphic fungus of the genus Sporothrix. It is considered a cosmopolitan disease, mainly in tropical and subtropical regions, and is endemic in Latin America [1]. In Brazil, there are two modes of transmission to humans: traumatic inoculation with contaminated soil and organic matter, and zoonotic transmission (infected felines) [1,2].
Sporotrichosis can be either cutaneous or extracutaneous, the former being more frequent. The cutaneous forms include lymphocutaneous, localized cutaneous and cutaneous by multiple inoculations. In the extracutaneous forms, various organs/systems can be affected, including the kidneys, lungs, heart and the ocular, nasal and genital mucosae, as well as the possibility of immunoreactive forms [3].
Classically, the disease manifests 2-4 weeks after the trauma as a papulonodular lesion at the inoculation site, most frequently located on the extremities in adult patients (sporotrichotic chancre), which may ulcerate and form fistulas. Nodules and gummas can appear and progress via lymphatic pathways (lymphangitis).
Itraconazole, potassium iodide, oral terbinafine and intravenous amphotericin B are the most commonly used drugs in Brazil for the treatment of sporotrichosis [1]. In the fixed cutaneous and lymphocutaneous variants, itraconazole is recommended as the first choice, even in immunosuppressed patients [1,4,5]. Potassium iodide was the initial treatment of choice for the lymphocutaneous and localized variants of sporotrichosis but it was later replaced by itraconazole due to easier dosing, although they present equivalent levels of efficacy and evidence. Notable side effects of potassium iodide include a metallic taste in the mouth and gastrointestinal intolerance symptoms [4,5]. Fluconazole is considered a second-line therapeutic option with inferior efficacy [4,6]. Amphotericin B deoxycholate, or preferably one of its lipid forms (lipid complex or liposomal), is the drug of choice for the treatment of severe and disseminated or life-threatening forms [1,4,7,8].
In the present report, we present an uncommon case of sporotrichosis manifesting on the face with a relatively atypical clinical presentation, which responded satisfactorily to treatment with potassium iodide.
Case presentation
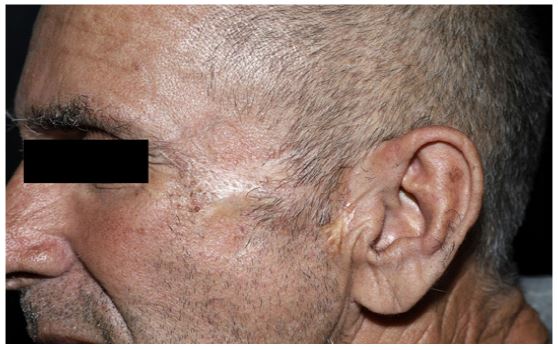
A 65-year-old male patient, a farm worker from the interior of São Paulo, Brazil, presented to the Dermatology Clinic of the Hospital das Clínicas, School of Medicine, University of São Paulo, reporting a verrucous lesion on his face for 4 months. He reported that the condition began after an accidental fall at his workplace, resulting in a facial injury. Following the fall, a small wart-like lesion appeared at the site, initially discharging purulent secretion. Upon seeking medical assistance, he was treated with oral and topical antibiotics for 15 consecutive days, but with no improvement. As the lesion progressed, he was referred to our clinic, where he presented with an erythematous-infiltrated plaque with verrucous and irregular borders, painful, approximately 4 cm in diameter, located in the left zygomatic region. On clinical examination, there were no mucosal lesions or regional lymphadenopathy (Figure 1).
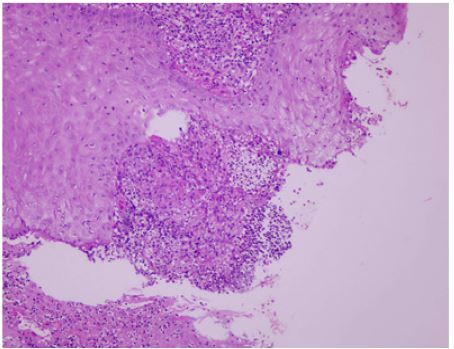
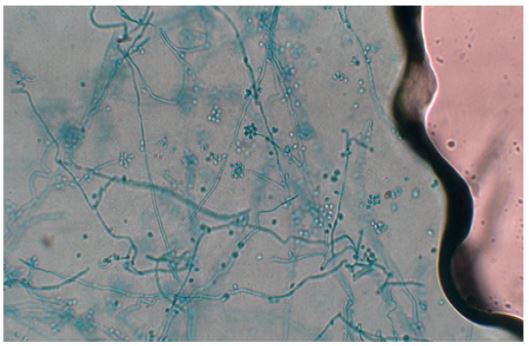
Skin fragments were collected from the lesion to establish a diagnosis. Direct mycological examination of the collected material was negative. Histopathological examination revealed suppurative granulomatous dermatitis with interspersed plasma cells, pseudoepitheliomatous hyperplasia, and neutrophilic exudation (Figure 2). Specific stains like Fite Faraco and Grocott did not demonstrate acid-fast bacilli or fungi, respectively. Fungal culture on Sabouraud dextrose agar with chloramphenicol at 25oC showed a whitish membranous colony with a blackened peripheral halo. Culture at 37oC exhibited a yeast-like appearance. Microscopic examination of the microculture revealed septate hyphae with conidiophores bearing conidia arranged in a bouquet-like formation at the apex, suggestive of infection by fungi of the genus Sporothrix (Figure 3). Molecular biology methods were not employed for species identification. Serological tests for syphilis, HIV, renal function evaluation, and blood glucose were normal or negative, but the patient tested positive for hepatitis C with normal liver enzymes.
Once the diagnosis of sporotrichosis was confirmed, treatment was initiated with potassium iodide in distilled water at a dose of 1 mg/kg/day. The medication was well tolerated, with the patient reporting only occasional metallic taste in the mouth, and there was no need to suspend or adjust the dose administered. Monthly outpatient visits were conducted for follow-up, and at the end of 6 months of treatment, the patient showed complete resolution of the lesion, prompting discontinuation of the medication (Figure 4). The patient has been followed in outpatient care for 5 months since the end of treatment without recurrence of the condition.

Discussion
Sporotrichosis exhibits a worldwide distribution with focal areas of hyperendemicity. It is particularly common in tropical/subtropical regions and temperate zones with warm and humid climates, which favor the growth of saprophytic fungi. However, large outbreaks have occurred in other locations as well [9,10]. Its global incidence is unknown, but Japan, China, Australia, Central and South America (Mexico, Brazil, Colombia, Peru), and India (along the Sub-Himalayan region) account for the majority of cases [11,12]. The disease is caused by dimorphic fungi of the genus Sporothrix, with 53 species currently recognized through phylogenetic analyses. The species most commonly associated with the disease include S. brasiliensis, S. schenckii, S. globosa and S. luriei, whose distributions vary geographically [13].
Infection typically occurs through traumatic inoculation of fungal fragments found in soil, plants and contaminated organic matter, or via zoonotic transmission. The presentation and clinical course of sporotrichosis are highly heterogeneous, depending on the site and method of inoculation, pathogen virulence, and host immune response. This variability makes diagnosis challenging, with multiple differential diagnoses, particularly in localized forms. Differential diagnosis should include chromoblastomycosis, American cutaneous leishmaniasis, paracoccidioidomycosis, cutaneous tuberculosis, squamous cell carcinoma, keratoacanthoma, and pyoderma gangrenosum [13-15].
Despite itraconazole being considered first-line treatment in adults and the elderly, our patient had a positive serology for hepatitis C. Therefore, potassium iodide was chosen for treatment, primarily due to its ease of administration. Our experience with potassium iodide has shown rapid resolution and cure of the disease, good safety, and low recurrence rates. Potassium iodide exhibits anti-inflammatory and immunomodulatory actions, inhibiting biofilm formation in both filamentous and yeast phases of the fungus [16-19].
Conclusion
The case presented highlights the importance of early and accurate diagnosis of verrucous lesions, particularly in elderly patients and those with lesions in sun-exposed areas, where differential diagnosis with neoplastic lesions and other relatively common deep mycoses in rural environments is imperative. The case also underscores the effectiveness of potassium iodide in treatment - a low-cost medication virtually free of side effects and easy to administer, allowing for outpatient management of the patient.
References
- Orofino-Costa R, Macedo PM, Rodrigues AM, Bernardes-Engemann AR. Sporotrichosis: an update on epidemiology, etiopathogenesis, laboratory and clinical therapeutics. An Bras Dermatol. 2017; 92: 606-20.
- Barros M, Schubach A, Schubach T, Wanke B, Lambert-Passos S. An epidemic of sporotrichosis in Rio de Janeiro, Brazil: Epidemiological aspects of a series of cases. Epidemiol Infect. 2008; 136: 1192-96.
- Bonifaz A, Tirado-Sánchez A. Cutaneous Disseminated and Extracutaneous Sporotrichosis: Current Status of a Complex Disease. J Fungi. 2017; 10: E6.
- Mahajan VK. Sporotrichosis: An Overview and Therapeutic Options. Dermatol. Res Pract. 2014; 2014: 272376.
- Costa RO, Macedo PM, Carvalhal A, Bernardes-Engemann AR. Use of potassium iodide in Dermatology: updates on an old drug. An Bras Dermatol. 2013; 88: 396-02.
- García-Carnero LC, Lozoya-Pérez NE, González-Hernández SE, Martínez-Álvarez JA. Immunity and Treatment of Sporotrichosis. J Fungi. 2018; 4:100.
- Verma S, Verma G, Rattan R. Lymphocutaneous Sporotrichosis of Face with Verrucous Lesions: A Case Report. Indian Dermatol Online J. 2019; 10: 303-06.
- Belda jr W, Passero LFD, Casolato ATS. Case Reports in Dermatological Medicine. 2021; 1-5
- D. Quintal. Sporotrichosis infection on mines of the Witwatersrand, Journal of Cutaneous Medicine and Surgery. 2000; 4(1): 51-54.
- D M Dixon, I F Salkin, R A Duncan et al. Isolation and characterization of Sporothrix schenckii from clinical and environmental sources associated with the largest U.S. epidemic of sporotrichosis, Journal of Clinical Microbiology. 1991; 29(6): 1106-1113.
- VK Mahajan, NL Sharma, RC Sharma, ML Gupta, G Garg et al. Cutaneous sporotrichosis in Himachal Pradesh, India, Mycoses. 2005; 48(1): 25-31.
- T De Araujo, AC Marques, F Kerdel. Sporotrichosis, International Journal of Dermatology. 2001; 40(12): 737-742.
- Orofino-Costa R, Freitas DFS, Bernardes-Engemann AR, Rodrigues AM, Talhari C, et al. Human sporotrichosis: recommendations from the Brazilian Society of Dermatology for the clinical, diagnostic and therapeutic management. An Bras Dermatol. 2022; 97(6): 757-777. doi: 10.1016/j.abd.2022.07.001.
- VK Mahajan, NL Sharma, V Shanker, P Gupta, K Mardi. Cutaneous sporotrichosis: unusual clinical presentations, Indian Journal of Dermatology, Venereology and Leprology. 2010; 76(3): 276-280.
- Barros, Mônica Bastos de Lima, et al. Sporothrix schenckii and Sporotrichosis. Clinical microbiology reviews. 2011; 24(4): 633-54. doi:10.1128/CMR.00007-11
- Belda Jr w, Chiacchio N, Criado P. Tratado de Dermatologia 4ª.Ed. Rio de Janeiro, Atheneu. 2023; 1524-32.
- Sharma B, Sharma AK, Sharma U. Sporotrichosis: A comprehensive review on recent drug-based therapeutics and management. Curr Dermatol Rep. 2022; 11: 110-9.
- Junior DS, Faria JRV, Carvalho CHC, Belda Jr W. Facial sporotrichosis by sporothrix brasiliensis in a pediatric patient. J Dermatol Res. 2023; 4: 1-4.
- Lyra Mr, Sokoloski V, de Macedo PM, Azevedo ACP. Sporotrichosis refractory to conventional treatment:therapeutic success with potassium iodide. An Bras Dermatol. 2021; 96: 231-3.