
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Basocellular carcinoma of atypical location
Walter Belda Junior*; Caroline Helena Chagas De Carvalho
Department of Dermatology, Faculty of Medicine, University of São Paulo, Brazil.
*Corresponding Author : Walter Belda Junior
Department of Dermatology, Faculty of Medicine, University of São Paulo, Brazil.
Email: [email protected]
Received : Jun 12, 2024
Accepted : Jun 25, 2024
Published : Jul 02, 2024
Archived : www.jcimcr.org
Copyright : © Belda Junior W (2024).
Abstract
Basal cell carcinoma is the most common malignant cutaneous tumor in humans. It can occur in any area of the body surface, but predominates in photo-exposed areas, particularly the face and trunk. Its main cause is chronic exposure over the years to ultra violet radiation, ionizing radiation, chemical carcinogens The occurrence of metastases is extremely rare. It has low mortality and extremely low metastatic rates (although when present, it indicates a poor patient prognosis); It also has a high morbidity rate through local destruction and recurrence, particularly when perineural invasion is observed, clinically or histopathologically.
We present a case of basal cell carcinoma of an atypical location on the lateral aspect of the thigh. The patient did not report or present any predisposing factors.
Keywords: Basal cell carcinoma; Atypical involvement; Basaloid carcinoma; Perineal carcinoma; Perineal.
Citation: Belda W, De Carvalho CHC. Basocellular carcinoma of atypical location. J Clin Images Med Case Rep. 2024; 5(7): 3150.
Introduction
Basal cell carcinoma, non-melanoma skin cancer, is the most common skin cancer in humans and its incidence corresponds to approximately 40% of cancers in general and 80% of non-melanoma skin cancers. It can be identified in any region of the skin surface [1-3], but more than 80% of lesions occur in photo-exposed areas, mainly the face and trunk. The mortality is low, but due to their high prevalence [4], BCC are a significant and costly health problem.
BCCs represent malignant tumors which have originated from basal cells found in the inter-follicular epidermis or in the hair follicle [5]. BCC cases further increase the burden to global cancer cases which are constantly on the rise; it is estimated that 1 in 5 males and 1 in 6 females will suffer from one form of cancer during their lifetime [6].
Basal cell carcinoma has low mortality and extremely low metastatic rates (although when present, it indicates a poor prognosis). However, it has a high morbidity rate, exemplified through local destruction and recurrence, particularly when Perineural Invasion (PNI) is present, allowing basal cell carcinoma to spread in a contiguous manner with secondary neuropathy. Extremely rare cases from the literature (11 in total) have reported basal cell carcinoma with intravascular invasion, having higher metastatic rates than basal cell carcinoma cases without this aggressive trait [7-10].
Case report
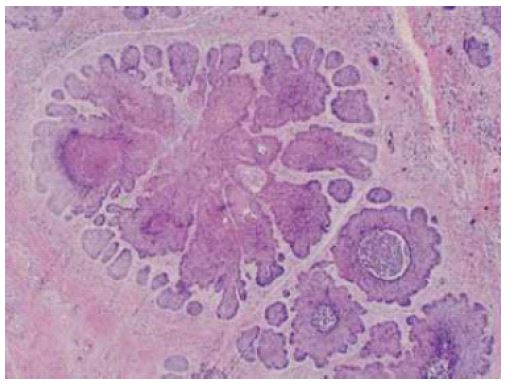
A 68-year-old man presented to our clinic with a growing lesion in the right inguinal region for the previous two years. Reports that the injury began as an abrasion and that it has been growing slowly and is painless. He reports that he is applying antibiotic cream with neomycin periodically, but without results. He informs that the lesion eventually bleeds. He denies the use of oral medications. He denies any history of sexually transmitted infections, exposure to arsenic or other chemicals. Denies the existence of an ulcerated or warty lesion at the site prior to the appearance of the current lesion. On clinical examination, the lesion was superficially ulcerated, measuring approximately 2 cm in diameter, with defined, shiny, pearly edges with discrete telagiectasias, an erythematous base, little infiltration, located on the inner side of the right thigh (Figure 1). No inguinal adenopathy. Despite the atypical location, the clinical hypothesis of basal cell carcinoma was made based on the clinical appearance of the lesion, and an anatomopathological examination was carried out to confirm the diagnosis. Histopathological examination: revealed tumoral infiltration consisting of basaloid cell nests causing superficial ulceration, with basaloid cells in a palisade in the periphery of the nests (Figure 2), confirming the clinical hypothesis of basal cell carcinoma. In view of the biopsy results, the patient underwent surgical excision of the lesion, made with a 3 cm margin, Histopathological examination of the excised lesion was also reported as basal cell carcinoma.

Discussion
Basal cell carcinoma is the most common skin tumor in humans. It is frequently seen in areas exposed to the sun, such as the head and neck region. The tumor is very slow-growing, and apart from exceptional circumstances, it does not metastase and is therefore one of the malignant tumors with the best courses [4]. The incidence basal cell carcinoma increases with age, and mean age at diagnosis is 68 years [11].
Superficial basal cell carcinoma are pink-red in color, squamous, and macule or patch-shaped, and the lesions may contain telangiectasia. The most commonly involved areas are the shoulders, chest or back, and multiple lesions may be present. Clinically, basal cell carcinoma may resemble inflammatory dermatoses such as eczema or psoriasis, and superficial basal cell carcinoma should be considered when permanent, erythematous, squamous lesions are encountered.
Histopathologically, the superficial subtype possesses small basaloid cell islets in the epidermis, with no dermal invasion. This is therefore the basal cell carcinoma with the best prognosis [12].
The most common causes of the development of basal cell carcinoma are ultra violet radiation, ionizing radiation and chemical carcinogens. Familial syndromes have been implicated in its development, such as nevoid basal cell carcinoma syndrome and xeroderma pigmentosum, Bazex syndrome, epidermolysis bullosa simplex, oculocutaneous albinism, Rombo syndrome along with immunodeiciencies, radiation infection, trauma, burns, and chronic irritation [13].
The etiological factors of basal cell carcinoma in unexposed areas are still unknown. In the present case presented no cause has been identified in terms of predisposing factors.
Conclusion
In conclusion, although basal cell carcinoma are seen in the head and neck region, they must also be considered in atypical locations. They should be considered in lesions resembling inflammatory dermatoses with a long-term history.
References
- Mohan SV, Chang AL. Advanced Basal Cell Carcinoma: Epidemiology and Therapeutic Innovations. Curr Dermatol Rep. 2014; 3: 40-5.
- Karagun E, Gamsizkan M, Eyup Y, Bahcivan A, Ozcan Y, BuyucekS. Atypically Located Basal Cell Carcinoma: Three Case Reports. Osmangazi Journal of Medicine. 2020; 42(3): 334-338.
- Saldanha G, Fletcher A, Slater DN. Basal cell carcinoma: a dermatopathological and molecular biological update. Br J Dermatol. 2003; 48: 195-202.
- Aldana PC, Yfantis HG, John PR. Perianal Basal Cell Carcinoma Successfully Managed with Excisional Biopsy. Case Rep Dermatol Med. 2019; 6268354.
- McCarthy W H, Shaw H M. Skin cancer in Australia Med J Aust. 1989;150: 469-470.
- Messina J, Epstein EH Jr, Kossard S, McKenzie C, Patel RM, Patterson JW and Scolyer RA: Chapter 1-Keratinocytic/epidermal tumors. Basal cell carcinoma. In: WHO Classification of skin tumors. Elder DE, Massi D, Scolyer RA and Willemze R (eds). 4th edition. International Agency for Research on Cancer, Lyon. 2017; 26-24.
- Poignet B, Gardrat S, Dendale R, Lemaitre S, Lumbroso-Le Rouic L, Desjardins L, et al: Basal cell carcinomas of the eyelid: Results of an initial surgical management. J Fr Ophtalmol. 2019; 42: 1094-1099.
- Kim DP, Kus KJB and Ruiz E: Basal cell carcinoma review. Hematol Oncol Clin North Am. 2019; 33: 13-24.
- Ashraf DC, Kalin-Hajdu E, Levin MH and Kersten RC: Mixed cranial neuropathies due to occult perineural invasion of basal cell carcinoma. Am J Ophthalmol Case Rep. 2018; 13: 136-139.
- Muzumdar S, Stewart CL and Feng H: Rare case of a basal cell carcinoma with intravascular invasion. Int J Womens Dermatol. 2020; 6: 334-335.
- Cameron MC, Lee E, Hibler BP, Barker CA, Mori S, Cordova M, Nehal KS, Rossi AM, et al. Basal cell carcinoma: Epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol. 2019; 80: 303-17.
- Cohen PR. Basal cell carcinoma of the axilla: review of the World literature. Am J Clin Dermatol. 2014; 15: 95-100.
- Paterson CA, Young-Fadock TM, Dozois R. Basal cell carcinoma of the perianal region: 20-year experience. Dis Colon Rectum. 1999; 42: 1200-2.