
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
How do we perform an open myomectomy?
Marcos de Lorenzo Messina; Alice de Paula Baer; Sophia Helena Batalha*; Ana Luísa Smith Rocha; Nicole Kemberly Ribeiro Rocha; Eduardo Vieira da Motta; José Maria Soares Júnior; Edmund Chada Baracat
Clinics Hospital University of São Paulo (USP-SP), Brazil.
*Corresponding Author : Sophia Helena Batalha
Clinics Hospital University of São Paulo (USP-SP), Brazil.
Email: sophiabatalha17@gmail.com
Received : Jun 13, 2024
Accepted : Jun 28, 2024
Published : Jul 05, 2024
Archived : www.jcimcr.org
Copyright : © Batalha SH (2024).
Abstract
31-year-old woman with symptomatic uterine fibroids who underwent open myomectomy. Despite prior treatment with goserelin, persistent symptoms and desire for future fertility warranted surgical intervention. The surgical technique aimed to optimize hemostasis and minimize morbidity by employing fusiform incisions.
Keywords: Uterine fibroids; Myomectomy; Misoprostol.
Citation: Messina MDL, Baer ADP, Batalha SH, Rocha ALS, Rocha NKR, et al. How do we perform an open myomectomy?. J Clin Images Med Case Rep. 2024; 5(7): 3155.
Introduction/Background
The aim of this study is to report a technique of an open myomectomy and its impacts on patients morbidity.
Methods: Medical record analysis and literature review at Scientific Database.
Case presentation
A 31-year-old woman presented to our clinic with heavy menstrual bleeding, anemia, and severe dysmenorrhea; she had no significant medical history and expressed a desire for future pregnancy. Pelvic ultrasound in September 2023 revealed an enlarged uterus with multiple uterine fibroids, with a total volume of 635 cc. The patient was initiated on goserelin 10.8 mg every 3 months for two doses, resulting in symptomatic improvement. Follow-up transvaginal ultrasound in January 2024 showed a slight reduction in uterine volume, to 563 cc, and the largest characterized fibroid measuring 9.0 x 7.5 cm. Due to the persistence of symptoms and the desire for future fertility, the patient was scheduled for surgical intervention and underwent an abdominal myomectomy, receiving 400 mcg of misoprostol vaginally one hour before the procedure to reduce blood loss. Preoperative hematimetric indices were Hemoglobin (Hb) 13.4. Post-surgery, her Hb levels were recorded as follows: 24 hours post-surgery: Hb 05/28: 11.4; and 48 hours later: Hb 10.9. His Histopathological examination of the excised tissue confirmed the presence of uterine leiomyomas without any concerning histological features.
Discussion/conclusion
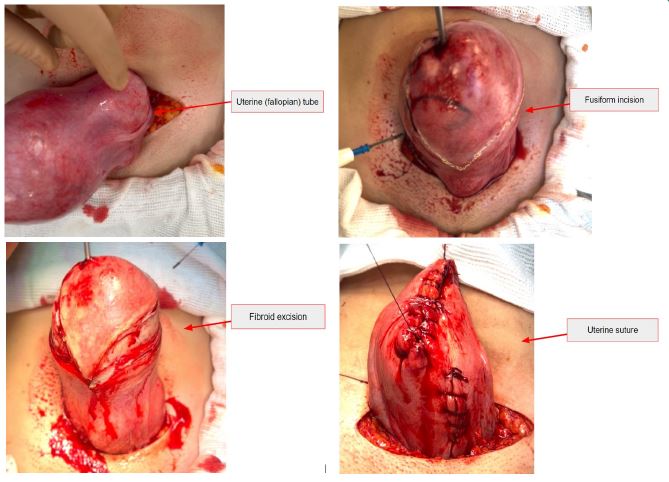
In patients that desire a reproductive future and that the tumor provides an alteration of the endometrial cavity the myomectomy plays a role. When it’s a submucous myoma, all guidelines suggest a surgical intervention (Figure 1). On the other hand, there is no consensus on what the best approach should be in intramural fibroids. In this patient of the study, we chose an open myomectomy with preoperative misoprostol one hour before the procedure to reduce blood loss, hemoglobin drop and blood transfusion [1-3]. The uterine incision through the myometrium in tumores above 4-5 centimeters was made in a fusiform shape to facilitate the approximation of the edges of the surgical wound and thus reduce closure time and consequently the bleeding. Despite multiple incisions that could increase the likelihood of adhesions, we see that attempting to extract multiple fibroids from a single incision could cause tunneling defects that could hamper hemostasis. Furthermore, it is important to have careful planning to avoid incising the cornua and fallopian tubes. The two-layer closure process with 0-Vycril suture provides adequate tissue apposition and increases the success of hemostasis. Thus we can reduce patients’ morbidity [4,5].
Acknowledgements: We would like to thank the patient for allowing us to share this clinical image that may inspire open myomectomy techniques providing greater success in hemostasis to reduce the morbidity.
References
- Wali S, Balfoussia D, Touqmatchi D, Quinn S. Misoprostol for open myomectomy: A systematic review and meta: Analysis of randomised control trials. Bjog: An International Journal of Obstetrics & Gynaecology, [S.L.]. Wiley. 2020; 128(3): 476-483. http://dx.doi.org/10.1111/1471-0528.16389.
- Michos G, Dagklis T, Papanikolaou E, Tsakiridis I, Oikonomou K, et al. Uterine Leiomyomas and Infertility: A Comparison of National and International Guidelines. Cureus. 2023; 15(12): e50992. doi: 10.7759/cureus.50992.
- Jeldu M, Asres T, Arusi T, Gutulo MG. Pregnancy Rate after Myomectomy and Associated Factors among Reproductive Age Women Who Had Myomectomy at Saint Paul’s Hospital Millennium Medical College, Addis Ababa: Retrospective Cross-Sectional Study. Int J Reprod Med. 2021; 2021: 6680112. doi: 10.1155/2021/6680112.
- Huerga López C, Gutiérrez Alagüero A, Cristóbal García I. Management of uterine fibroids: Approach to medical treatment. Med Clin (Barc). 2023; 161(Suppl1): S15-S21. doi: 10.1016/j.medcli.2023.06.035
- Alkhrait S, Malasevskaia I, Madueke-Laveaux OS. Fibroids and Fertility. Obstet Gynecol Clin North Am. 2023 Dec;50(4):663-675. doi: 10.1016/j.ogc.2023.08.006. Epub 2023 Oct 3. PMID: 37914486.