
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Unusual parapharyngeal lipoma
Ibtissam Larhrabli*; Naanani Othmane; Loudghiri M; Bijou W; Oukessou Y; Rouadi S; Abada RL;
Roubal M; Mahtar M
ENT Head and Neck Surgery Department, Ibn Rochd University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
*Corresponding Author : Ibtissam Larhrabli
ENT Head and Neck Surgery Department, Ibn Rochd University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
Email: bettylar92@gmail.com
Received : Jun 13, 2024
Accepted : Jun 28, 2024
Published : Jul 05, 2024
Archived : www.jcimcr.org
Copyright : © Larhrabli I (2024).
Abstract
Less than 1% of head and neck malignancies are Parapharyngeal Space (PPS) tumors; salivary gland tumors make up the majority, followed by tumors with a neurogenic origin [1]. Despite being the most prevalent benign mesenchymal tumors of the head and neck, lipomas are not frequently seen in the PPS [2]. Larger PPS lesions are reached through an infratemporal fossa or combination transcervical-transmandibular route, although the majority of lesions are approached transcervically [3,4]. According to published research, PPS lipomas are restricted to either the prestyloid or poststyloid compartments. We report a unique case of lipoma involving the two PPS compartments [5,6].
Citation: Larhrabli I, Othmane N, Loudghiri M, Bijou W, Oukessou Y, et al. Unusual parapharyngeal lipoma. J Clin Images Med Case Rep. 2024; 5(7): 3156.
Description
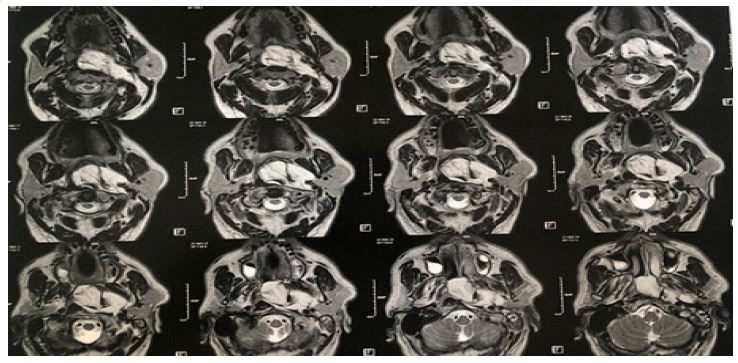
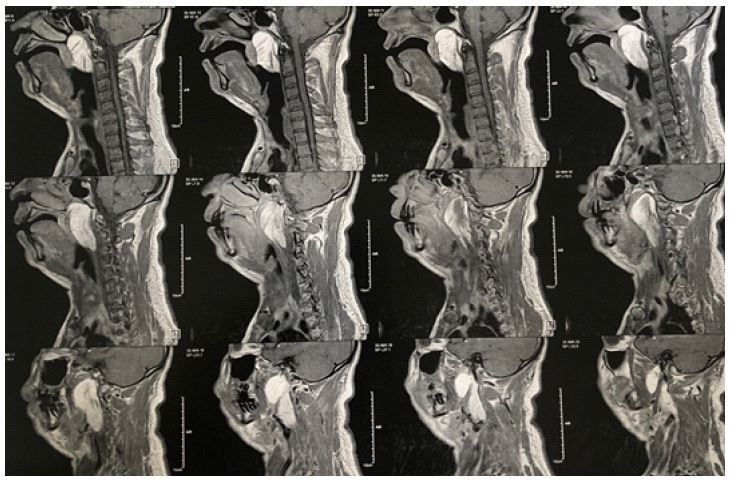
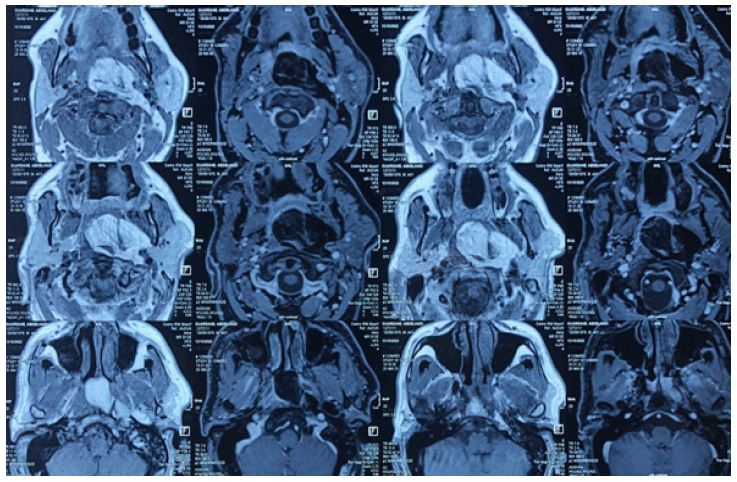
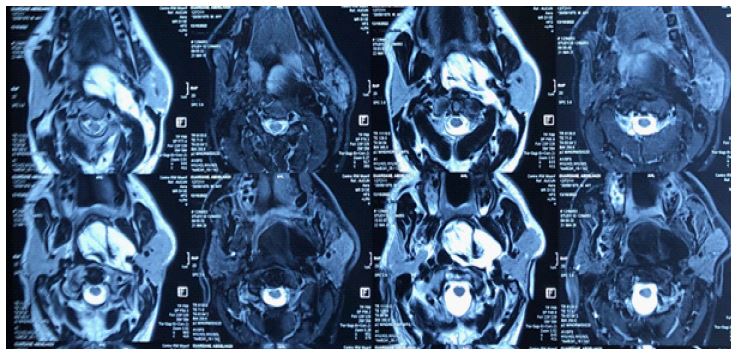
We report a case of a 51 year-old male presented in our departement with complaints of change in voice since six months and difficulty in swallowing solids since 1 month, difficulty in breathing when sleeping on his back. In physical examination on intra-oral cavity, a 7 x 5 cm smooth, soft, spherical bulge was noted over the right lateral wall of the oropharynx obstructing nearly 90% of the luminal space, displacing the tonsil medially and reaching the nasopharynx superiorly. Indirect laryngoscopy showed the lesion reaching up to the superior edge of the epiglottis. The MRI revealed an extensive and well-limited expansive process of fatty component in franc hypersignal T1 and T2 (Figures 1 & 2) which disappears on the sequences in fat saturation (Figures 3 & 4), extended over 92 x 40 mm on the sagittal plane and 60 x 27 mm on the axial plane.
The patient underwent excision of the lesion by a both oral and transcervical approach under general anesthesia. A horizontal incision was made in the neck crease 2 finger breadth below the mandible. A level II dissection was done to expose the carotid sheath contents and delineate the hypoglossal nerve. The facial vessels were ligated and submandibular gland mobilized anteriorly. The stylohyoid muscle and posterior belly of the diagastric were divided to facilitate exposure superiorly till the skull base. The lesion was dissected from adjacent tissues by a combination of blunt and sharp dissection, retracting the carotid vessels anterolaterally and hypoglossal nerve superiorly. Histopathological evaluation showed mature adipocytes interspersed with fibrous tissue, confirming the diagnosis of Lipoma. Post-operatively, the patient did not present any complications, remains symptom-free with complete recovery of neuromuscular function.
Declarations
Patient consent: Consent to publish the case report was obtained.
Funding: No funding or grant support.
Authorship: All authors attest that they meet the current ICCRR criteria for Authorship.
References
- Ulku CH, Uyar Y. Parapharyngeal lipoma extending to skull base: a case report and review of the literature. Skull Base. 2004; 12: 121-125. doi: 10.1055/s-2004-828708.
- Carrau RL, Myers EN, Johnson JT. Management of tumors of the parapharyngeal space. Oncology. 1997; 11: 633-640.
- Smith JC, Snyderman CH, Kassam AB. Giant parapharyngeal space lipoma: case report and surgical approach. Skull Base. 2002; 12:215-220. doi: 10.1055/s-2002-35754-1.
- Singh PP, Sharma A, Gupta N. Parapharyngeal space lipoma. Ind J Otolaryngol Head Neck Surg. 2004; 56: 152-154.
- Abdullah BJJ, Liam CK, Kaur H, Mathew KM. Parapharyngeal space lipoma causing sleep apnea. Br J Radiol. 1997; 70: 1063-1065. doi: 10.1259/bjr.70.838.9404213.