
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Case of dilated cardiomyopathy after cellular therapy
Latipbayeva MS*; Askarov MB; Seisembekov TZ; Aktanova GE
National Scientific Medical Research Center JSC, Astana 010000, Kazakhstan.
*Corresponding Author : Latipbayeva MS
National Scientific Medical Research Center JSC, Astana 010000, Kazakhstan.
Tel: +77-013130888;
Email: meru_27_92@mail.ru
Received : Jun 14, 2024
Accepted : Jul 01, 2024
Published : Jul 08, 2024
Archived : www.jcimcr.org
Copyright : © Latipbayeva MS (2024).
Abstract
Dilated cardiomyopathy is an etiologically heterogeneous myocardial disease characterized by left ventricular or biventricular dilation with systolic dysfunction in the absence of hemodynamic overload factors (hypertension, valvular defects, congenital heart anomalies) or coronary pathology (ischemic heart disease) [1]. Dilated cardiomyopathy can develop at any age but is more common in young people. About 10% of those who develop Dilated cardiomyopathy are over 65 years old [2]. Studies have shown that optimal medication therapy is insufficiently effective for patients with idiopathic dilated cardiomyopathy [4]. Thus, there was a need to develop alternative approaches and methods for the treatment of chronic heart failure. One of these methods is cellular technology [5]. A large number of clinical studies have been published, mainly using stem cells derived from bone marrow as injectable cells. Clinical trials conducted on patients with chronic heart failure have expanded understanding and shown that cell therapy is safe and effective [7].
We present a clinical case of a 41-year-old female patient with dilated cardiomyopathy who underwent autologous bone marrow cell transplantation six years ago due to a low left ventricular ejection fraction. According to echocardiography and magnetic resonance imaging, the left ventricular ejection fraction was 19%, and the heart chambers were dilated.
In 2018, the patient first complained of shortness of breath during physical exertion, palpitations and swelling in the lower extremities after a viral infection. The patient received optimal drug therapy for heart failure for six months, but there was no positive dynamics. She was then sent to the National Scientific Medical Research Center for cellular therapy.
A year after the cell transplantation, the echocardiography and magnetic resonance imaging showed an increase in left ventricular ejection fraction to 51%. Currently, the patient feels satisfactory and reports no complaints of shortness of breath or heart palpitations.
Keywords: Dilated cardiomyopathy; Chronic heart failure; Left ventricular ejection fraction; Cell therapy; Autologous bone marrow; Pro-BNP; Brain natriuretic peptide.
Citation: Latipbayeva MS. Case of dilated cardiomyopathy after cellular therapy. J Clin Images Med Case Rep. 2024; 5(7): 3158.
Clinical case
Patient T., female, born in 1977. Complains of shortness of breath and attacks of palpitations during physical exertion (fast walking), decreased exercise tolerance, swelling in the lower extremities.
According to the patient, at the age of 41, after suffering an acute respiratory viral infection, she first experienced complaints of shortness of breath, decreased tolerance to physical activity, and swelling in the lower extremities. She consulted at the local clinic, underwent examination, and Echocardiography (EchoCG) showed a Left Ventricular Ejection Fraction (LVEF) of 19%. The cardiologist prescribed optimal medication therapy: tab. Stopress 4 mg, 1 tab once a day; tab. Carvedilol 6.25 mg, 1 tab twice a day; tab. Espiro 25 mg, 1 tab once a day; tab. Torsid 5 mg, 1 tab. once a day. Despite the regular intake of the above-mentioned drugs, the patient’s condition gradually worsened in the form of an increase in shortness of breath, increased heart palpitations, increased swelling and the appearance of cough. As a result, the patient was referred to the cardiology clinic at “NSMRC” JSC in Astana for examination and treatment. On 10.04.2018, she was hospitalized in the cardiology department. Coronary angiography was performed, revealing no pathology of the coronary arteries. The patient was offered cell transplantation. According to the selection criteria, the patient was included in the research program “Study of the effectiveness and safety of transplantation of multipotent autologous mesenchymal bone marrow cells in patients with chronic heart failure” in the control group.
Denies tuberculosis, viral hepatitis, skin-venereal diseases. An increase in Blood Pressure (BP) of more than 120/80 mmHg is not noted, an adapted BP of 100/70 mmHg.
Allergy history: Not burdened. No bad habits. Denies surgeries, injuries, blood transfusions. Heredity: not burdened by cardiovascular diseases.
Upon admission, the general condition was of moderate severity due to Heart Failure (HF). The severity of HF was assessed using the 6-minute walk test according to the New York Heart Association (NYHA) classification.
Skin: Pale. Peripheral lymph nodes are not enlarged, mobile, painless, and not matted. Thyroid gland: not enlarged on palpation. Musculoskeletal system: no pathological changes. Breasts are normally developed. Marked edema from feet to the mid-third of the shins on both sides. Body temperature: 36.4°C. Weight: 73 kg. Height: 158 cm. Body Mass Index (BMI): 29 kg/m².
Respiratory system: Breathing through the nose is free. The chest is symmetrical, with both halves participating equally in breathing. Breathing is rhythmic and of normal depth. Respiratory Rate (RR): 20 per minute. On palpation, the chest is painless. Voice trembling is moderate over symmetrical areas of the chest. Percussion sound over the lungs is clear. Auscultation of the lungs: breathing is harsh, weakened in the lower parts. No rales. No crepitation. No pleural friction rub.
Cardiovascular system: On examination of the neck and heart area, no pathological pulsations. The apex beat is intensiintensified, shifted leftward and downward. The heart impulse is not palpable. Heart sounds: muffled, rhythmic.
Murmurs: Systolic murmur at the apex of the heart. Heart Rate (HR): 80 per minute. BP left arm: 110/70 mmHg. BP right arm: 110/70 mmHg. Pulse: 80 beats per minute, symmetrical, satisfactory filling and tension.
Digestive system: Tongue moist and clean. Abdomen soft and painless. Liver at the edge of the rib arch. Spleen not palpable. Stool regular and formed.
Urinary system: Negative Pasternatsky symptom on both sides. Urination is free and painless.
Quality of life assessment using the Minnesota questionnaire: 70 points – this indicator corresponds to an average level of life satisfaction in the patient.
Six-minute walk test: 250 m, corresponding to the third functional class of HF.
Risk of venous thromboembolism: 4 points - low molecular weight heparins and unfractionated heparin in prophylactic dose.
Results
Slight decrease in hemoglobin: 116 g/L, increased Erythrocyte Sedimentation Rate (ESR): 22 mm/h, increased NT-proBNP: 2432 pg/mL, hypercholesterolemia: Total cholesterol: 7.27 mmol/L, other analyses within normal limits: Leukocytes: 5.17x10⁹/L, Platelets: 298x10⁹/L, C-reactive protein: 2 mg/L, Creatinine: 79 μmol/L, Urea: 3.6 mmol/L, Potassium: 4.5 mmol/L, Sodium: 141 mmol/L, Calcium: 1.3 mmol/L, ALT: 0.29 μkat/L, AST: 0.23 μkat/L, Glucose: 4.9 mmol/L, CD73: 10 U/L, CD4: 30 U/L, CD8: 24 U/L, CD34: 1 U/L.
Instrumental methods of examination (10.04.2018)
Electrocardiogram (ECG): sinus rhythm, HR 79 bpm. Electrical axis of the heart deviated to the left. PQ interval: 0.2 s; QRS duration: 0.11 s.
Chest X-ray: Lung pattern fine reticulated in the lower parts, cardiac shadow expanded to the left.
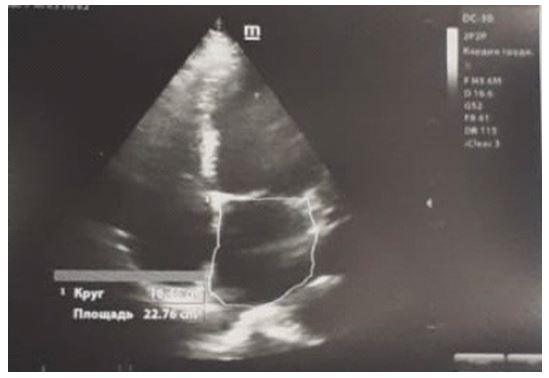
Echocardiography (EchoCG): Aortic root: 23 mm, Left Atrium (LA): 50 mm, right ventricle (RV): 33 mm, Ascending Aorta: 28 mm, End-Diastolic Volume (EDV): 182 mm, End-Systolic Volume (ESV): 123 mm, End-Diastolic Dimension (EDD): 65 mm, end-systolic dimension (ESD): 58 mm, LVEF: 25%. Systolic function of the left ventricle is reduced. Dilatation of the left heart chambers, slightly of the right atrium. Mitral regurgitation grade 3, tricuspid regurgitation grade 1.5. Global contractility of the left ventricle is reduced. Pulmonary artery systolic pressure (PASP): 48 mmHg (Figure 1).
Cardiac MRI: MRI findings of reduced global contractile function of the left ventricular myocardium. LVEF: 19% (endocardial volume) and 25% (blood volume). Diffuse hypokinesis of the left ventricular walls. Dilatation of all heart chambers. Mitral insufficiency grade 4. Reduced stroke volume (404-427 mL), decreased cardiac output (38-40 L/min), and cardiac index (22-24 mL/m²).
Based on the patient’s history, physical examination, and laboratory and instrumental findings, the clinical diagnosis is established:
Clinical diagnosis: Primary disease: Dilated cardiomyopathy DCM.
Complication of the primary disease: CHF NYHA Class III.
Mitral insufficiency grade 4.
Concomitant disease: Familial hyperlipoproteinemia Fredrickson type IIb.
Treatment: Treatment of heart failure according to the European Society of Cardiology guidelines: Diet No. 10. Tablets Sacubitril/valsartan 50 mg twice a day, tablets Carvedilol 25 mg a day, tablets Eplerenone 50 mg a day, tablets Torasemide 5 mg a day, tablets Atorvastatin 20 mg, Enoxaparin sodium injection 0.4 mL once a day.
Operation (16.04.2018): The patient underwent puncture of the posterior third of the iliac crest (using a fixed needle for bone marrow extraction VME 13/7; 13G x 7 cm Gallini Medical Devices, Italy) with the exfusion of 200 mL of bone marrow. In the stem cell biotechnology laboratory, the mononuclear (hematopoietic) fraction of stem cells was isolated, with pre-cultivation of autologous MSCs for 17-18 days. After counting viable cells, the mononuclear MSC fraction (70-100x10⁶) was administered intravenously in 200 mL of physiological solution at a rate of 50 mL/h.
Discharge (17.04.2018): After discharge, the patient was monitored by a cardiologist and continued standard HF therapy.
The patient was under cardiologist observation and received inpatient treatment every 3 months. At the first inpatient visit after MSC transplantation, an improvement in quality of life and increased tolerance to physical activity was noted.
The clinical condition of the patient was assessed using the NYHA classification functional class and the 6-minute walk test. The HF functional class corresponded to NYHA Class II.
Quality of life was assessed using a validated method – the Minnesota Living with Heart Failure Questionnaire.
At the last visit, 9 months later, the patient’s condition was satisfactory with no complaints. During follow-up, a statistically significant increase in LVEF from 25% to 51% and a decrease in EDV from 182 to 98 mL, and ESV from 123 to 34 mL were observed. The pro-BNP level decreased significantly compared to baseline. Tolerance to physical activity improved according to the NYHA classification of HF severity, which decreased from Class III to Class I.
Table 1: Pro-BNP indicators and NYHA functional class of heart failure.
| Indicators | 1st visit | 2nd visit | 3rd visit |
|---|---|---|---|
| PRO-BNP | 2432 pg/mL | 7,18 pg/mL | 7 pg/mL |
| CHF class according to NYHA | III | II | I |
*Note: Pro-BNP: Brain Natriuretic Peptide; NYHA: New York Heart Association.
On ECG: Sinus rhythm, HR 71 bpm. The electrical axis of the heart is deviated to the left. ST segment is on the isoelectric line.

Follow-up after MSC transplantation (9 months): At the second hospitalization, no complaints, no dyspnea on exertion, no peripheral edema. General condition satisfactory. Body temperature: 36.4°C. Weight: 73 kg. Height: 158 cm. BMI: 29 kg/m². Heart sounds rhythmic. HR: 70 bpm. BP: 110/80 mmHg.
Laboratory and instrumental follow-up data: No increase in immunological parameters (interleukins (IL-4, IL-10, IL-1 beta, TNF-2 beta)). Pro-BNP decreased to 7 pg/mL.
Table 2: The course of endoscopic treatments.
| Indicators | Before | After |
|---|---|---|
| LVEF (endocardial volume) | 19% | 42% |
| LVEF (blood volume) | 25% | 51% |
| LVEDD | 69 mm | 58 mm |
| LVESD | 59 mm | 38 mm |
| EDV | 208 mL | 120 mL |
| ESV | 168 mL | 69 mL |
*Note: MRI: Magnetic Resonance Imaging; LVEF: Left Ventricular Ejection Fraction; LVEDD: Left Ventricular End-Diastolic Dimension; LVESD: Left Ventricular End-Systolic Dimension; EDV: End-Diastolic Volume; ESV: End-Systolic Volume.
ECG (Figure 1) Sinus rhythm, HR 71 bpm. The electrical axis of the heart is deviated to the left. ST segment is on the isoelectric line.
EchoCG (Figure 3) LA: 4.0 cm, RV: 2.4 cm, LVEDD: 59 mm, LVESD: 42 mm, EDV: 144 mL, ESV: 84 mL, LVEF: 51%. Slight dilation of the left ventricle and left atrium. Local myocardial contractility of the ventricles is preserved. Global contractility of the left ventricle is slightly reduced.
Control Cardiac MRI (Table 2) after 1.5 years (18.10.2019) MRI findings of increased global contractility of the left ventricular myocardium (LVEF: 42% (endocardial volume) and 51% (blood volume)), increased stroke volume (467/502 mL), and cardiac output (32/34 L/min). Mitral insufficiency grade 3. Quality of life and tolerance to physical activity improved. The functional class of HF severity decreased from Class III to Class I. LVEF increased significantly (Table 1).
Conclusion
Based on the above clinical case, it can be concluded that the transplantation of autologous mesenchymal bone marrow cells in combination with optimal medication therapy for CHF leads to an improvement in the overall and local contractile function of the myocardium and positively affects the patient’s quality of life. The use of cell preparations for the treatment of DCM is one of the promising and developing treatment methods.
References
- Perry Elliott, Bert Andersson, Eloisa Arbustini, Zofia Bilinska, Franco Cecchi: Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008; 29(2): 270-6.
- Tisha Suboc: Dilated cardiomyopathy: N Engl J Med. 2022; 331: 1564-1575.
- Bojan Vrtovec, Gregor Poglajen, Luka Lezaic, Matjaz Sever, Dragoslav Domanovic, Peter Cernelc, Aljaz Socan, Sonja Schrepfer: Effects of intracoronary CD34+ stem cell transplantation in nonischemic dilated cardiomyopathy patients: 5-year follow-up. Circ Res, 2013; 112(1): 165-73.
- O.L. Nikiforova, L.N. Prikhodko, P.N. Kovalchuk: Clinical observation of a patient with chronic heart failure after mesenchymal stem cell implantation in outpatient practice. Health and Ecology Issues. 2021; 18(2): 131-139.
- Robert E. Michler, et al. Stem Cell Therapy for Heart Failure; Methodist DeBakey Cardiovasc J. 2013; 9(4): 187-194.