
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Vulvar leiomyosarcoma: A clinical image
Marcos de Lorenzo Messina; Eduardo Vieira da Motta; Gabriela Natania Sales Rebelo*; Andre Luis Costa Ennes; Dariane Sampaio Alves Morales Piato; José Maria Soares Júnior; Jesus de Paula Carvalho; Edmund Chada Baracat
Department of Obstetrics and Gynecology, Clinical Hospital University of São Paulo, Brazil.
*Corresponding Author : Gabriela Rebelo
Department of Obstetrics and Gynecology, Clinical Hospital University of São Paulo, Brazil.
Email: gabriela.rebelo@hc.fm.usp.br
Received : Jun 15, 2024
Accepted : Jul 02, 2024
Published : Jul 09, 2024
Archived : www.jcimcr.org
Copyright : © Rebelo GNS (2024).
Keywords: Vulvar mass; Vulvar leiomyosarcoma.
Citation: Messina ML, Motta EV, Rebelo GNS, Ennes ALC, Piato DSAM. Vulvar leiomyosarcoma: A clinical image. J Clin Images Med Case Rep. 2024; 5(7): 3160.
Description
Objective: To report a case of vulvar leiomyosarcoma.
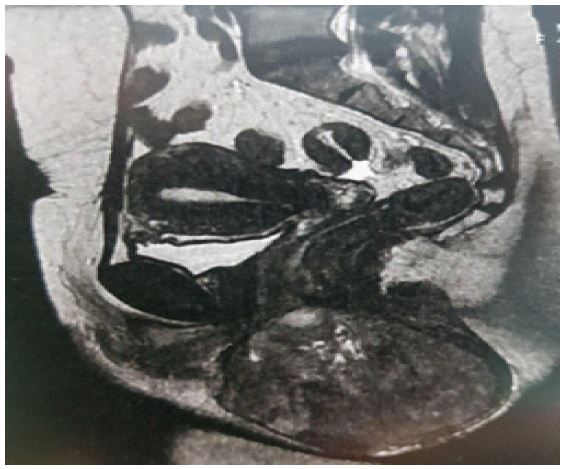
Methods: Medical record analysis and literature review at scientific Database. MP, a 48-year-old female, presented with a 3-month history of a ten-centimeter vulvar mass on the left major labia, adhered to a deep plane, and associated with local pain (Figure 1). There was no history of perineal trauma or pruritus. A magnetic resonance image showed a 10.7 x 8.5 x 10.7 cm lesion, with a solid component, well-defined contours, no cleavage plane, and constricting the anorectal region (Figure 2).
At first, a punch biopsy was performed showing a benign result. An excision biopsy was done (Figure 3), resulting in a grade 2 leiomyosarcoma with angiolymphatic invasion, mitotic index of 12 mitosis per high power field (Figure 4).
Since staging thoracic computerized tomography showed lung suspicious nodes and retroperitoneal enlarged lymph nodes, chemotherapy sessions were indicated. During the treatment, a swelling aspect on the surgical site aroused suspicion for local recurrence. A magnetic resonance reviewed a slight increase in tumoral mass. A left hemivulvectomy with margin ampliation was performed, followed by radiotherapy sessions. After evidence of progression of lung suspicious nodes, palliative chemotherapy was indicated. Patient died secondary to pneumonia two months later.


Discussion
Vulvar sarcomas are rare neoplasms, the clinical presentation is frequently confused with benign conditions, such as Bartholin’s gland conditions [1]. Suspicions may arise in cases of fast-growing vulvar enlargements, with or without ulceration, or in those cases adherent to a deep perineal plane [2].
Given the similarity of clinical presentations, enlargements in the major labia glands, with an atypical development course, especially in patients over 40 years old, might necessitate a biopsy [3].
A punch biopsy and other incisional biopsy modalities may not be accurate enough to diagnose vulvar sarcomas. Wide local excision as the first surgical approach seems to be suitable, as resection with microscopically negative margins is related to a reduced recurrence risk [4]. A 1-2 cm resection margin is considered optimal, although it is important to consider the increase in morbidity that this margin size might imply.
Lymphadenectomy is not routinely performed since it does not seem to reduce the recurrence risk [5].
References
- Reinicke T, Anderson DJ, Kumar D, Griggs C. Vulvar Leiomyosarcoma Masquerading as a Bartholin’s gland Cyst in an Adolescent. Cureus. 2022; 14.
- Verta S, Alwafai Z, Schleede N, Brambs CE, Christmann C, et al. Vulvar Leiomyosarcomas: A Case Series with Clinical Comparison to Uterine Leiomyosarcomas and Review of the Literature. Am J Case Rep. 2023; 27: 24
- Aartsen EJ, Albus-Lutter CE. Vulvar sarcoma: clinical implications. Eur J Obstet Gynecol Reprod Biol. 1994; 56: 181-189.
- Akrivi S, Varras M, Anastasiadi Z, Pappa C, Vlachioti A, et al. Primary vulvar leiomyosarcoma localized in the Bartholin’s gland area: A case report and review. Mol Clin Oncol. 2021; 14: 69.
- Shankar S, Todd PM, Rytina E, Crawford RA. Leiomyosarcoma of the vulva. J Eur Acad Dermatol Venereol. 2006; 20: 116-7.