
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A case with respiratory failure caused from iatrogenic hypercalcemic crisis
Ismail Ozer1; Adem Dirican2; Turkan Mete3; Tuba Ciftci4; Doga Ozkaya5; Sevket Ozkaya6*
1Internal Medicine and Nephrologist, Samsun VM Medical Park Hospital, Department of Internal Medicine, Samsun, Turkey.
2Pulmonologist, Assistant Professor, Altinbas University, Faculty of Medicine, Department of Pulmonary Medicine, Istanbul, Turkey.
3Internal Medicine and Endocrinologist, Samsun VM Medical Park Hospital, Department of Internal Medicine, Samsun, Turkey.
4Pulmonologist, Assistant Professor, Altinbas University, Faculty of Medicine,Department of Pulmonary Medicine, Istanbul, Turkey.
5Medical Student, Palacky University, Faculty of Medicine, Olomuc, Czech Republic.
6Pulmonologist, Professor, Altinbas University, Faculty of Medicine, Department of Pulmonary Medicine, Istanbul, Turkey.
*Corresponding Author : Sevket Ozkaya
Professor, Altinbas University, Faculty of Medicine, Department of Pulmonary Medicine, Istanbul, Turkey.
Tel: +90 532 4741309;
Email: ozkayasevket@yahoo.com
Received : Jun 10, 2024
Accepted : Jul 03, 2024
Published : Jul 10, 2024
Archived : www.jcimcr.org
Copyright : © Ozkaya S (2024).
Abstract
Hypercalcemia is a critical and urgent clinical condition that can lead to death, related to blood calcium levels. We present a case of a 69-year-old female who presented with respiratory and renal failure, depression due to iatrogenic hypercalcemia developing in a patient using uncontrolled calcium and vitamin D.
Keywords: Calcium; Iatrogenic Hypercalcemia; Respiratory failure.
Citation: Ozer I, Dirican A, Mete T, Ciftci T, Ozkaya S, et al. A case with respiratory failure caused from iatrogenic hypercalcemic crisis. J Clin Images Med Case Rep. 2024; 5(7): 3163.
Introduction
Calcium is one of the most important, common and critical minerals in human body. Normally, human body carefully controls the level of calcium in blood, but certain medications and conditions such as excessive use of calcium and vitamin D for therapeutic purposes can result in high blood calcium levels [1]. Hypercalcemia is a critical and urgent clinical condition that can lead to death, related to blood calcium levels. We present a case of a 69-year-old female who presented with respiratory and renal failure, depression due to iatrogenic hypercalcemia developing in a patient using uncontrolled calcium and vitamin D.
Case presentation
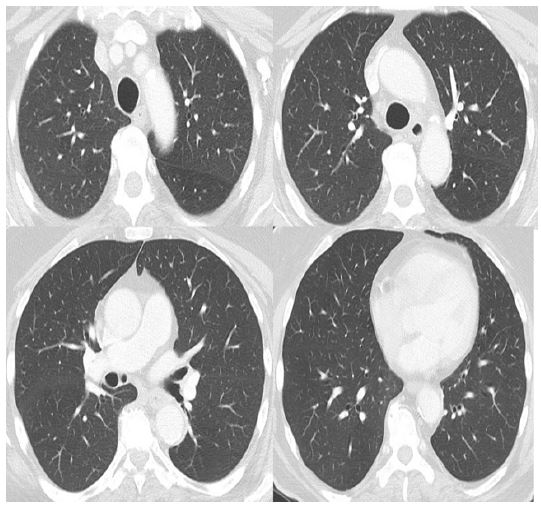
A 69-year-old female patient presented in the emergency and neurology departments of our hospital with chronic cough, dyspnea, weakness, nause, altered mental status, depression findings. She had a history of controlled diabetes mellitus and arterial hypertension. Also, she was diagnosed with arthritic symptoms with hypocalsemia 1 year ago and was treated with calcium supplements and vitamin D analogs. 1 year prior to her admission, she was found to have serum Calcium of 8.4 mg/dL (normal range 8.8-10.2 mg/dL), serum creatinine 1.1 mg/dL (normal range 0.1-0.9 mg/dL) and thoracic CT images were normal (Figure 1).
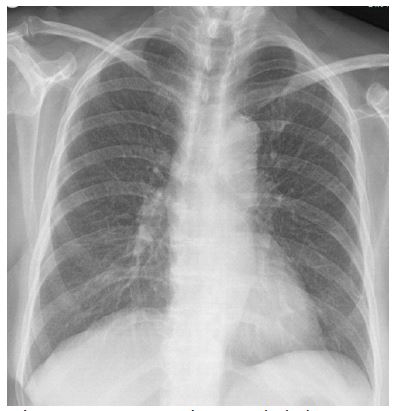
Calcium supplements and vitamin D analogs were prescribed and she did not have medical control with the continued the uncontrolled dosages of these drugs by herself. On admission she was confused and hypoxemic. There was no acute abnormality on Brain MRI and Echocardiography. COVID 19 test was negative. There was no significant findings on clinical examination and chest roentgenography is looked like normal (Figure 2).
Calcium supplements and vitamin D analogs were prescribed and she did not have medical control with the continued the uncontrolled dosages of these drugs by herself. On admission she was confused and hypoxemic. There was no acute abnormality on Brain MRI and Echocardiography. COVID 19 test was negative. There was no significant findings on clinical examination and chest roentgenography is looked like normal (Figure 2).
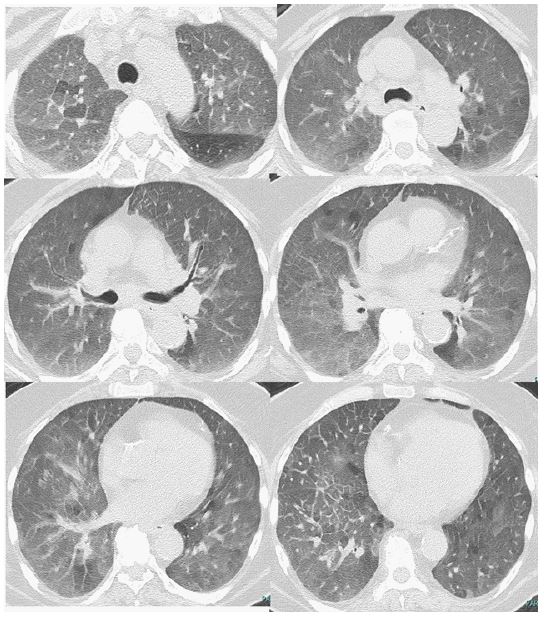
Thoracic CT performed because of hypoxemia and it showed that the bilaterally diffuse ground-glass attenuation with septal thickening (Figure 3).
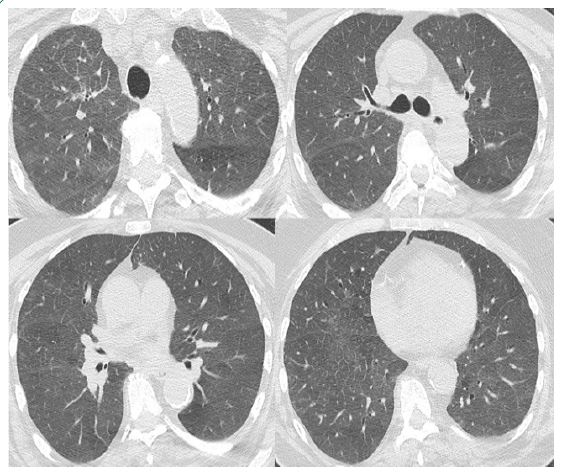
Laboratory tests; serum Calcium 15.8 mg/dL (normal range 8.8-10.2 mg/dL), serum creatinine 1.7 mg/d L(normal range 0.1-0.9 mg/dL), Parathyroid Hormon 4.25 ng/L (normal range 15-65 ng/L) and 25-OH Colecalsiferol vitamin D3 61 μg/L (normal range 30-75 μg/L) and SaO2 85% on pulse oximetry. She was treated with intravenous fluids, furosemid, corticosteroid, zoledronic acid and oxygen therapy with discontinuation of calcium supplements and vitamin D analogs. After the 4 days, patient’s clinical and radiologic status improved and serum Calcium and serum creatine decreased at the level of 8.8 mg/dL and 1.3 mg/dL, respectively. The diffuse ground glass opacities were gradually decreased on HRCT with the treatment (Figure 4).
Discussion
According to published case reports, we did not find a case like us with hypoxemic respiratory failure due to diffuse lung damage caused from iatrogenic hypercalcemia. All of the reported cases, pulmonary involvement in patients with hypercalcemia caused from primary hyperparathyroidism (PHPT) or malignancy. Also, like in our case ARDS (Acute Respiratory Disstress Syndrome) is a very rare complication of hypercalcemic crisis, especially in the clinical course of PHPT, since most cases are associated with malignancies [2-6]. Holmes et al. were the first to describe a case of ARDS in a patient with parathyroid crisis in 1974 [3]. The prevalence of hypercalcemia in the general population is approximately 1% to 2%. Most of the cases (90%) of hypercalcemia are due to primary hyperparathyroidism and malignancy-associated hypercalcemia. Hypercalcemia is classified into mild hypercalcemia (10.5 to 11.9 mg/dL), moderate hypercalcemia (12.0 to 13.9 mg/dL), and hypercalcemic crisis (14.0 to 16.0 mg/dL). Iatrogenic hypercalcemia is a disorder rarely described in literature and there are few reported cases of association with pulmonary complication. Abnormal physical symptoms and complications are usually observed with a serum calcium level above 12 mg/dl. Apart from pulmonary infections and sepsis, cardiogenic pulmonary edema should always be excluded, as hypercalcemia may trigger cardiac arrhythmias and accelerate vascular and valvular calcification. In our case, cardiac rhythm and functions were normal despite the severe hypercalsemia. The pathophysiological mechanism involved in the induction of acute lung injury in hypercalcemic crisis remains elusive. In the case reported by Holmes et al., autopsy revealed extensive calcium deposition in the alveolar cells and the authors suggested that probably this depositions destroyed alveolar/capillary barrier leading to lung injury [3]. An experimental study in conscious rats and isolated perfused rat’s lungs, performed by Chen et al., suggested that hypercalcemia may produce a sepsis-like syndrome and acute lung injury by increasing plasma nitrate/nitrite, free radicals, proinflammatory cytokines, procalcitonin and iNOS activity [7].
Chest roentgenography usually seen normal in hypercalsemic cases, just like in our case. There may be ground-glass appearances on Thoracic CT images, that cannot be detected on chest radiography, as in our patient. We think that lung involvement in a hypercalcemic patient is directly proportional to calcium levels. Like in our case, the rapid clinical, laboratory and radiological response is achieved with the stan-dard treatment of hypercalcemia as intravenous fluids, furosemide, corticosteroid, and zoledronic acid.
Conclusion
In conclusion; as the first case with diffuse lung involvement caused from iatrogenic hypercalcemia developing in a patient using uncontrolled calcium and vitamin D, every patient with symptoms due to hypercalcemia should be evaluated in detail for pulmonary complications.
Declarations
Competing interests: No potential conflict of interest was reported by the authors.
Authors contributions: AD, SO, TM, IO and TC contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript. SO and AD contributed to the patients care. DO contributed to the design of figures and collection of datas. All authors have read and agreed to the published version of the manuscript.
Funding statement: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- Lafferty FW. Differential diagnosis of hypercalcemia. J Bone Miner Res. 1991; 6 (12): 51-9.
- Hsu YH, Chen HI. Acute respiratory distress syndrome associated with hypercalcemia without parathyroid disorders. Chin J Physiol. 2008; 51: 414-418.
- Holmes F, Harlan J, Felt S, Ruhlen J, Murphy B. Pulmonary oedema in hypercalcaemic crisis. Lancet. 1974; 303: 311-312. 10.1016/s0140-6736(74)92615-4.
- Mert M, Uzuncan FB, Aydin MM, Kocabay G, Ortakoylu A. A hyperparathyroid case with pulmonary edema: can hypercalcemia trigger pulmonary edema?. Am J Emerg Med. 2012; 30: 512. 10.1016/j.ajem.2010.12.033.
- Wymenga AN, van der Werf TS, van der Graaf WT, Tulleken JE, Zijlstra JG, Ligtenberg JJ. Lessons from an unusual case: malignancy associated hypercalcemia, pancreatitis and respiratory failure due to ARDS. Neth J Med. 1999; 54: 27-30. 10.1016/s0300-2977(98)00077-1.
- Poe RH, Kamath C, Bauer MA, Qazi R, Kallay MC, Woll JE. Acute respiratory distress syndrome with pulmonary calcification in two patients with B cell malignancies. Respiration. 1989; 56: 127-133.
- Chen HI, Yeh DY, Kao SJ: The detrimental role of inducible nitric oxide synthase in the pulmonary edema caused by hypercalcemia in conscious rats and isolated lungs. J Biomed Sci. 2008; 15: 227-238.