
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Findings on temporal lobe epilepsy confused with panic disorder
Deniz Yildiz1; Emre Aydin2*
1Specialist Psychiatrists Private Clinic Bandirma, Balikesir, Turkey.
2Department of Neurology, Bandirma Onyedi Eylül University, Faculty of Medicine, Balikesir, Turkey.
*Corresponding Author : Emre Aydin
Department of Neurology, Bandirma Onyedi Eylül University, Faculty of Medicine, Balikesir, Türkey.
Email: eaydin@bandirma.edu.tr
Received : May 29, 2024
Accepted : Jul 04, 2024
Published : Jul 11, 2024
Archived : www.jcimcr.org
Copyright : © Aydın E (2024).
Abstract
Panic disorder symptoms may be confused with temporal lobe epilepsy findings. In this study, it was determined that the complaints of an male adult patient with panic disorder for 4 years were associated with temporal lobe epilepsy. Partial-onset seizures presenting with panic attack symptomatology can pose a diagnostic challenge. It will be beneficial for clinicians to keep in mind the sensory seizure due to epilepsy while taking the case history of panic symptoms.
Keywords: Panic; Epilepsy; Temporal lobe.
Citation: Yildiz D, Aydin E. Findings on temporal lobe epilepsy confused with panic disorder. J Clin Images Med Case Rep. 2024; 5(7): 3165.
Introduction
Panic disorder (PD) is a disorder that affects quality of life with symptoms such as chest tightness, palpitations, shortness of breath, sweating, tremor, chills, numbness, loss of balance, nausea, or abdominal pain [1]. There are publications that the rate of PD increases up to 5% in life-long studies [2]. As in other anxiety disorders, people with panic disorder may think that they have a problem, and the time to apply to the clinic may increase, and this may delay the treatment [3]. Fear, an affective symptom associated with idiopathic panic attacks, is also seen as an ictal symptom in 10-15% of patients with temporal lobe epilepsy [4]. Temporal lobe epilepsy [TLE] is a complex, neuropsychiatric disorder in which the neurological presentation may be complicated by various emotional, behavioural, or personality abnormalities, and can sometimes be confused with the findings of panic disorder. The clinical distinction between simple partial epileptic seizures originating from the temporal lobe and panic attacks is often difficult on a stand-alone clinical basis. Because both conditions are characterized by a common symptomatology including a feeling of fear, autonomic system dysfunction, disorientation, and changes in the level of consciousness [5]. Causes of TLE include mesial temporal sclerosis, cortical dysplasia, tumour, vascular malformation, ischemia, infection, and trauma. In some of the temporal lobe epilepsies, no pathology may be demonstrated [6]. The fact that up to 20% of patients diagnosed with epilepsy have normal electroencephalography [EEG], even when monitored with video-EEG, further complicates the difficulty in diagnosis [7].
Case presentation
In this case study, a rare case of a male patient with temporal lobe epilepsy who thought he had panic disorder but did not receive treatment for 4 years will be presented. A 41-year-old male patient applied to a psychiatrist for mental confusion, feeling of “sugar” in the mouth and tremors, which he described as “malaria” which he felt sometimes every 6 months and sometimes once a month, up to 4-5 times a day. In his history, it was learned that he had previously applied to a psychiatrist with a diagnosis of panic disorder and used “Escitalopram 10 mg”. He stated that he noticed an increase in the signs of tremor with the use of antidepressant medication. The patient stated that he had ignored the findings that he had previously considered as panic, and that these findings had started 4 years ago.
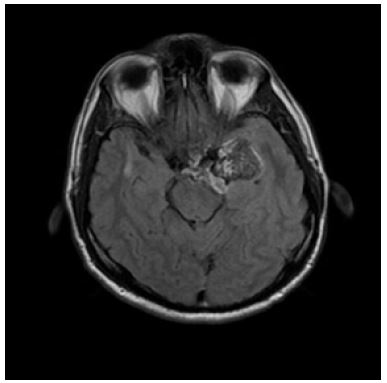
Since the patient’s mental state examination did not reveal any active psychopathological findings and his symptoms, which he described as panic attack, were not accompanied by anxiety symptoms, the patient was referred to neurology with the preliminary diagnosis of sensory seizure. The EEG findings of the patient who was referred to neurology were found to be normal. On MRI, a 36 x 35 mm lesion in the widest part of the insular cortex of the left temporal region was seen with a slightly hyperintense appearance in T1W series and with contrast enhancement in postcontrast series. It was reported that the described lesion was evaluated as associated with epidermoid cyst. The lesion creates pressure on the mesencephalon in the right posteromedial (Figure 1). It was understood that the panic-like symptoms experienced by the patient were sensory seizures. The patient was referred to the neurosurgery department for operation.
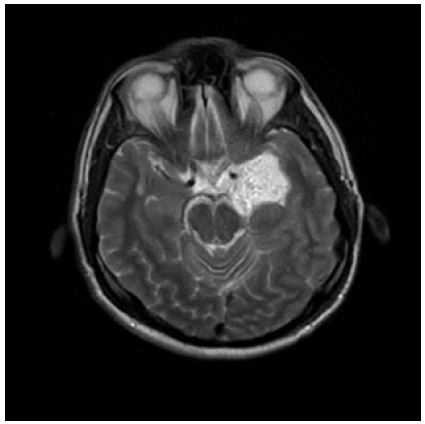
The epileptic focus area was successfully removed from the left anterior temporal lobe and has been seizure-free since. In addition, he did not describe the putative symptoms of panic attacks (Figure 2).
Discussion
In the literature, there are reported cases of panic disorder and temporal lobe epilepsy presenting to a psychiatrist, as in this case [8-10]. While an epidermoid cyst was detected in our case, it was reported that temporal lobe epilepsy, which was confused with panic disorder in previous case reports, was caused by causes such as arteriovenous malformation, meningioma, and neurocysticercosis [11-13]. Fear has been described as the most common experiential phenomenon produced by direct electrical brain stimulation in temporal lobe epilepsy, localized in the anteromedial temporal region, including the amygdala. It may present with autonomic symptoms such as focal seizures and panic attacks, tachycardia, blood pressure fluctuations, hyperventilation, and shortness of breath.
Hemispheric control of autonomic function has been the subject of debate for many years. Despite some conflicting results in the literature, few researchers have demonstrated right hemisphere dominance for sympathetic heart rate and blood pressure modulation. The main region of autonomic representation in the brain is thought to include the insular cortex. There are papers suggesting that the spread of right mesial temporal ictal activity to the insular cortex may be responsible for autonomic panic attack symptomatology [14]. However, in our patient, a tumour was detected in the left temporal lobe. When panic is the only obvious symptom of epilepsy, the diagnosis and effective management of epilepsy can be seriously adversely affected medically and psychosocially, and patients may remain untreated for years. This case demonstrates that the diagnosis of simple partial seizures is sometimes difficult and can be confused with psychiatric conditions. Therefore, the physician—especially the psychiatrist—must be careful when treating panic attacks when they occur with atypical symptomatology or do not respond to properly selected therapy, as in this case. If possible, EEG and high-resolution MRI may be required for accurate diagnosis and treatment with a multidisciplinary approach. In this case report, it is aimed to raise awareness of the physician about the possibility of sensory epileptic seizures in patients presenting with panic disorder.
References
- Amerikan Psikiyatri Birliği, Psikiyatride Hastalıkların Tanımlanması ve Sınıflandırılması Elkitabı, Beşinci Baskı (DSM-5), Amerikan Psikiyatri Birliği, Washington DC, 2013’den çeviren Köroğlu E, Hekimler Yayın Birliği, Ankara, 2013.
- Auerbach RP, Mortier P, Bruffaerts R, Alonso J, Benjet C, Cuijpers P, et al. RCWHO World Mental Health Surveys International College Student Project: Prevalence and distribution of mental disorders. WHO WMH-ICS Collaborators. J Abnorm Psychol. 2018; 127(7): 623-638. doi: 10.1037/abn0000362. Epub 2018 Sep 13. PMID: 30211576
- Altamura, AC, Camuri, G, Dell’Osso, B. Duration of untreated illness and duration of illness in anxiety disorders: assessment and influence on outcome. Mod Trends Pharmacopsychiatry. 2013; 29: 111–118.
- Cendes F, Andermann F, Gloor P, et al. Temporal lob epilepsisinde amigdala atrofisi ile iktal korku arasındaki ilişki. Beyin 1994; 117: 739-46.
- Sazgar M, Carlen PL, Wennberg R. Epileptic Disord. 2003; 5(2): 93-100.
- Engel JJ, Shewmon D: Overview. Who should be considered a surgical candidate. In: Engel J (ed), Surgical Treatment of the Epilepsies, ikinci basım, New York: Raven Press Ltd., 1993: 23-34.
- T.M. Alsaadi et al. Video-EEG telemetry can be a crucial tool for neurologists experienced in epilepsy when diagnosing seizure disorders Seizure. 2004.
- Fraser-Rini J, Ochoa J. Panic Attack as the Sole Manifestation of Epilepsy Localized to the Nondominant Temporal Region. J Neuropsychiatry Clin Neurosci. 2020; 32(3): 309-311. doi: 10. 1176/appi.neuropsych.19070158.
- Lesional Temporal Lobe Epilepsy: Beware the Deceitful “Panic Attack”.Kulason KO, Schneider JR, Rahme R, Pramanik B, Chong D, Boockvar JA. World Neurosurg. 2018; 111: 197-200. doi: 10.1016/j.wneu.2017.12.124. Epub 2017 Dec 28.PMID: 29288854
- Hurley RA, Fisher R, Taber KH. Sudden onset panic: epileptic aura or panic disorder? J Neuropsychiatry Clin Neurosci. 2006; 18(4): 436-43. doi: 10.1176/jnp.2006.18.4.436.
- Wall M, Tuchman M, Mielke D. Panic attacks and temporal lobe seizures associated with a right temporal lobe arteriovenous malformation: case report.
- Scalise A, Placidi F, Diomedi M, De Simone R, Gigli GL. Panic disorder or epilepsy? A case report. J Neurol Sci. 2006; 246(1-2): 173-5. doi: 10.1016/j.jns.2006.02.017. Epub 2006 Apr 17. PMID: 16603192
- Ramos-Zúñiga R, Pérez-Gómez HR, Gaytán-Martínez LA, Vega-Ruiz B, Soto-Rodríguez S, Rochín-Mozqueda Sistiserkoz. Temporal lobe epilepsy and active neurocysticercosis: two representative case reports.
- Sazgar M, Carlen PL, Wennberg R. Panic attack semiology in right temporal lobe epilepsy. Epileptic Disord. 2003; 5(2): 93-100. PMID: 12875952.