
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Intracanalicular vestibular schwannoma: A case report
Moujrid S*; Hamza G; Bijou W; Oukessou Y; Rouadi S; Abada R; Roubal M; Mahtar M
ENT Department, Averroes University Hospital Casablanca, Morocco.
*Corresponding Author : Sara Moujrid
ENT Department, Averroes University Hospital Casablanca, Morocco.
Email: saramoujrid9@gmail.com
Received : May 30, 2024
Accepted : Jul 05, 2024
Published : Jul 12, 2024
Archived : www.jcimcr.org
Copyright : © Moujrid S (2024).
Abstract
Vestibular schwannomas (VS) are benign tumors that originate in the Schwann sheath of the vestibular nerve and constitute 6-8% of primary intracranial tumors. Intracanalicular vestibular schwannomas (IVS) are rare entities, usually identified by MRI, and they arise from the intracanal route and progress toward the cerebellopontine angle. Various factors contribute to this incidence, including increased cell phone use and increased use of diagnostic MRI. The Koos grading scale is used to categorize tumor progression. Clinical manifestations of vestibular schwannomas range from hearing loss to facial paralysis, with standard diagnostic approaches involving audiometry and gadolinium-enhanced MRI. Treatment modalities include observation, surgery, and stereotactic radiotherapy (SRS). For smaller vestibular schwannomas, observation is often the preferred approach, and SRS has been shown to be effective in both tumor control and hearing preservation.
Intracanalicular schwannoma presents as a distinctive clinical entity, requiring comprehensive evaluations such as MRI, pure-tone and speech audiometry, and vestibular assessment. SRS appears to be a very effective option, providing excellent control of tumor growth. It’s about a case study concerns a 65-year-old patient with a history of right seromucous otitis and who presented with progressive right hypoacusis. Clinical examinations and audiometry revealed left unilateral sensorineural hearing loss. MRI identified a 0.7 cm mass affecting the right acoustic nerve. Despite recommendations for surgical excision, the patient chose close monitoring as the next course of action.
Keywords: Intracanalicular vestibular neurinoma; Sensorineural deafness; Cerebellopontine angle.
Citation: Moujrid S, Hamza G, Bijou W, Oukessou Y, Rouadi S, et al. Intracanalicular vestibular schwannoma: A case report. J Clin Images Med Case Rep. 2024; 5(7): 3167.
Introduction
Vestibular schwannomas (VS) are histologically benign tumors that originate in the Schwann sheath of the vestibular nerve, a critical branch of the cochleovestibular nerve [1]. Representing approximately 6-8% of all primary intracranial tumors, 25-33% of posterior cerebral fossa tumors, and 75-86% of lesions in the cerebellopontine angle, these tumors exhibit slow growth and are typically diagnosed in individuals between the ages of 45 and 60, with a higher incidence observed in women [2,4].
While they commonly arise sporadically and unilaterally, bilateral occurrences are often associated with neurofibromatosis type 2, underscoring the significance of genetic factors in certain cases. The advent of magnetic resonance imaging (MRI) has significantly increased the detection rate of intracanalicular vestibular schwannomas (IVS), shedding light on this previously rare entity. IVS presents unique challenges and considerations in terms of diagnosis and management. Various treatment options are available for IVS, ranging from a conservative wait-and-see approach to more active interventions such as microsurgical resection or radiosurgery [5].
This article aims to contribute to the understanding of vestibular schwannomas by presenting a case study involving a patient who sought medical attention due to progressive left hearing loss. The subsequent diagnostic workup revealed the presence of an intracanalicular vestibular schwannoma, emphasizing the clinical relevance of early detection and appropriate management strategies for this rare condition.
Case report
This 65-year-old patient has a medical history that includes surgery performed five years ago for seromucous otitis on the right side. The reason for the current consultation is progressive hypoacusis on the right side, with no reported otalgia, otorrhea, vertigo, facial paralysis, or tinnitus. Otoscopic examination of the affected side revealed a permeable external ear canal with a remodeled appearance of the eardrum and tympanosclerosis. In contrast, the contralateral side appeared normal.
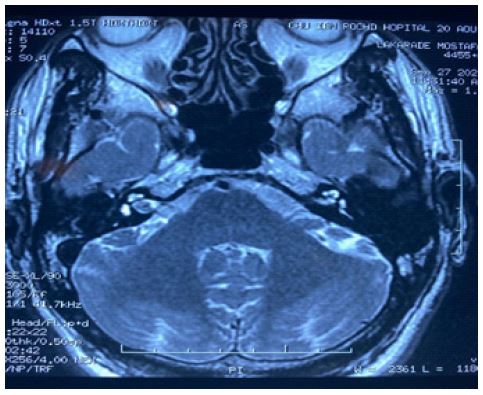
An audiogram with impedancemetry was conducted, revealing sensorineural deafness with a hearing loss of 65 dB, and a Rinne test result of 10 dB. Stapedial reflexes were present. Further assessment was pursued through an MRI of the ponto-cerebellar angle, identifying a small 0.7 cm mass affecting the acoustic nerve on the right side (Figure 1), confirmed to be a neuroma. Subsequently, vestibular Head Impulse Test (vHIT) and Video Nystagmography (VNG) were requested to explore the semicircular canals, and no anomalies were detected.
Given the diagnosis of a neuroma, the patient was advised for surgical excision, and the potential complications of the procedure were thoroughly explained. However, the patient opted against surgery and choose close monitoring of the pathology as the preferred course of action. It is noteworthy that this decision aligns with current literature, where the management of vestibular schwannomas can vary based on patient preferences, tumor size, and other individual factors.
Discussion
Vestibular schwannomas initially manifest as purely intraductal tumors, progressing subsequently to the cerebellopontine angle, and constituting approximately 95% of tumors found in the internal auditory canal [6]. These tumors originate from the myelin-producing Schwann cells within the vestibular portion of the vestibulocochlear nerve [7]. The global incidence of vestibular schwannomas is on the rise, currently ranging from 1 to 20 cases per million [8]. Various factors have been studied as potential contributors to this increase, including the heightened use of mobile phones and the overuse of diagnostic magnetic resonance imaging (MRI) studies [9,12].
The benign natural history of vestibular schwannomas, characterized by either no growth or slow growth at a rate of 1 to 2 mm per year [13,14], further contributes to their increasing prevalence. Estimates suggest a prevalence of around 200 cases per million [15].
The progression of vestibular schwannomas is classified using the Koos grading scale [16], providing a structured framework to understand the severity and evolution of these tumors. This scale assists clinicians in categorizing the tumors based on their size, extension, and involvement of surrounding structures, aiding in the formulation of appropriate management strategies (Table 1).
Regarding clinical signs, intra-canal vestibular schwannomas typically present with unilateral hearing loss, tinnitus, and balance issues. Larger extra-canal lesions may lead to trigeminal neuralgia, facial paralysis, cerebellar dysfunction, or even compression of the brainstem [17].
Table 1: Koos grading scale [16].
| Koos grade | Description |
|---|---|
| I | Intracanalicular tumor |
| II | Minimal tumor extension into the cerebellopontine angle, < 3 cm |
| III | Tumor occupies the cerebello-pontine angle but does not displace the cerebellar trunk, < 3cm |
| IV | Large tumor with brainstem displacement, ˃3 cm |
Hearing evaluation involves audiometric tests, with pure-tone audiometry and speech audiometry routinely performed during patient follow-up [18]. The Gardner Robertson classification, which combines average tonal hearing loss and speech discrimination score, is widely utilized for hearing assessments [19]. While audiometry has limited diagnostic value, it allows for the assessment of auditory function.
In terms of imaging, gadolinium-enhanced MRI of the head is the standard diagnostic approach for detecting vestibular schwannomas up to 2 mm in diameter [20]. The features observed on imaging are highly sensitive and specific, enabling an accurate radiological diagnosis in most cases, often eliminating the need for confirmatory biopsy [20,21].
Screening MRI studies are recommended in cases of sudden or asymmetric sensorineural hearing loss detected by tonal and speech audiometry [18]. The treatment objective is to prevent the functional consequences of tumor expansion while preserving the nerves of the cerebellopontine angle. Therapeutic management options range from active surveillance to surgery and radiotherapy, with regular clinical and radiological monitoring required once the treatment choice is made.
For smaller vestibular schwannomas, an observation period is often suggested, with surgery or radiosurgery considered only when tumor progression is confirmed by imaging. Stereotactic radiotherapy (SRS) is frequently chosen as the initial treatment for patients with small-volume vestibular schwannomas, offering high control of tumor growth with minimal risk to cranial nerve function and hearing. Studies have reported improved tumor control rates and hearing preservation rates with SRS compared to observation alone [23,24].
Microsurgical resection is the treatment of choice for larger tumors associated with symptomatic brainstem compression, hydrocephalus, trigeminal neuralgia, neuropathy, or a combination of these complications [20,26]. The 2019 European Association of Neuro-Oncology (EANO) guidelines recommend both observation and SRS as management options for small vestibular schwannomas, emphasizing the goals of controlling tumor growth, avoiding surgical risks, and preserving neurological function [25]. Observation remains the preferred management for small asymptomatic tumors with regular cranial nerve function. For small tumors with auditory and/or vestibular symptoms, SRS is favored due to its better rate of hearing preservation and lower risk of facial paresis compared to surgery. For tumors with complete hearing loss, SRS remains the primary therapeutic option [25].
Conclusion
Intracanalicular schwannoma stands out as a distinct clinical entity, characterized by its clinical presentation involving vestibular signs, acoustic disturbances, and neurophysiological effects, which should prompt immediate consideration of MRI.
For the comprehensive evaluation of vestibular schwannomas (VS), essential examinations include MRI, tonal and vocal audiometry, and vestibular assessment. These diagnostic modalities contribute to a thorough understanding of the tumor’s characteristics and its impact on auditory and vestibular functions.
Stereotactic Radiosurgery (SRS) emerges as a highly effective option for managing intracanalicular schwannomas, demonstrating excellent control over tumor growth. This minimally invasive therapeutic approach has proven to be successful in ensuring optimal tumor control, underlining its significance in the overall management strategy for these tumors.
References
- Microchirurgie du schwannome vestibulaire : les interrogations persistantes - em consulte
- Samii M, Gerganov VM. Tumors of the cerebellopontine angle. Handb Clin Neurol. 2012; 105: 633‑9.
- Briggs RJ, Fabinyi G, Kaye AH. Current management of acoustic neuromas: review of surgical approaches and outcomes. J Clin Neurosci Off J Neurosurg Soc Australas. 2000; 7(6): 521‑6.
- Posterior Cranial Fossa Meningiomas - Disponible sur: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3424023/
- Carlson ML, Link MJ. Vestibular Schwannomas. N Engl J Med. 2021; 384(14): 1335‑48.
- Yang BQ, Yang XL, Wu ZY, Wang L, Ren J, Wang WJ, et al. [Rare tumor of internal auditory canal]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 7 juill 2022; 57(7): 843‑7.
- Harner SG, Laws ER. Clinical findings in patients with acoustic neurinoma. Mayo Clin Proc. 1983; 58(11): 721‑8.
- Tos M, Stangerup SE, Cayé-Thomasen P, Tos T, Thomsen J. What is the real incidence of vestibular schwannoma? Arch Otolaryngol Head Neck Surg. févr 2004; 130(2): 216‑20.
- Stangerup SE, Tos M, Caye-Thomasen P, Tos T, Klokker M, Thomsen J. Increasing annual incidence of vestibular schwannoma and age at diagnosis. J Laryngol Otol. 2004; 118(8): 622‑7.
- Hardell L, Hansson Mild K, Sandström M, Carlberg M, Hallquist A, Påhlson A. Vestibular schwannoma, tinnitus and cellular telephones. Neuroepidemiology. 2003; 22(2): 124‑9.
- Howitz MF, Johansen C, Tos M, Charabi S, Olsen JH. Incidence of vestibular schwannoma in Denmark, 1977-1995. Am J Otol. sept 2000; 21(5): 690‑4.
- Wolbers JG, Dallenga AH, Mendez Romero A, van Linge A. What intervention is best practice for vestibular schwannomas? A systematic review of controlled studies. BMJ Open. 2013; 3(2): 001345.
- Arthurs BJ, Fairbanks RK, Demakas JJ, Lamoreaux WT, Giddings NA, Mackay AR, et al. A review of treatment modalities for vestibular schwannoma. Neurosurg Rev. 2011; 34(3): 265‑77; 277-279.
- Hajioff D, Raut VV, Walsh RM, Bath AP, Bance ML, Guha A, et al. Conservative management of vestibular schwannomas: third review of a 10-year prospective study. Clin Otolaryngol Off J ENT-UK Off J Neth Soc Oto-Rhino-Laryngol Cervico-Facial Surg. 2008; 33(3): 255‑9.
- Lin D, Hegarty JL, Fischbein NJ, Jackler RK. The prevalence of «incidental» acoustic neuroma. Arch Otolaryngol Head Neck Surg. 2005; 131(3): 241‑4.
- Koos WT, Day JD, Matula C, Levy DI. Neurotopographic considerations in the microsurgical treatment of small acoustic neurinomas. J Neurosurg. Mars. 1998; 88(3): 506‑12.
- Tringali S, Dubreuil C, Zaouche S, Ferber-Viart C. Are stage IV vestibular schwannomas preoperatively different from other stages? Otol Neurotol Off Publ Am Otol Soc Am Neurotol Soc Eur Acad Otol Neurotol. 2008; 29(1): 46‑9.
- Hadjipanayis CG, Carlson ML, Link MJ, Rayan TA, Parish J, Atkins T, et al. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines on Surgical Resection for the Treatment of Patients With Vestibular Schwannomas. Neurosurgery. 2018; 82(2): 40.
- Gardner G, Robertson JH. Hearing preservation in unilateral acoustic neuroma surgery. Ann Otol Rhinol Laryngol. 1988; 97(1): 55‑66.
- Dunn IF, Bi WL, Mukundan S, Delman BN, Parish J, Atkins T, et al. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines on the Role of Imaging in the Diagnosis and Management of Patients With Vestibular Schwannomas. Neurosurgery. 2018; 82(2): 32.
- Kim DH, Lee S, Hwang SH. Non-contrast Magnetic Resonance Imaging for Diagnosis and Monitoring of Vestibular Schwannomas: A Systematic Review and Meta-analysis. Otol Neurotol. 2019; 40(9): 1126.
- Ogino A, Lunsford LD, Long H, Johnson S, Faramand A, Niranjan A, et al. Stereotactic radiosurgery as the first-line treatment for intracanalicular vestibular schwannomas. J Neurosurg. 2021; 135(4): 1051‑7.
- Kaul V, Cosetti MK. Management of Vestibular Schwannoma (Including NF2): Facial Nerve Considerations. Otolaryngol Clin North Am. 2018; 51(6): 1193‑212.
- Regis J, Carron R, Park MC, Soumare O, Delsanti C, Thomassin JM, et al. Wait-and-see strategy compared with proactive Gamma Knife surgery in patients with intracanalicular vestibular schwannomas. J Neurosurg. Déc. 2010;113: 105‑11.
- Goldbrunner R, Weller M, Regis J, Lund-Johansen M, Stavrinou P, Reuss D, et al. EANO guideline on the diagnosis and treatment of vestibular schwannoma. Neuro-Oncol. 2020; 22(1): 31‑45.
- Trigeminal neuralgia and neuropathy in large sporadic vestibular schwannomas in: Journal of Neurosurgery. 2017; 127: 5. Disponible sur: https://thejns.org/view/journals/j-neurosurg/127/5/article-p992.xml.