
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Insights from a unique presentation of small cell neuroendocrine carcinoma of the paranasal sinuses: A case report
Nermin Abozenah*; Boris A Stuck; Richard Birk; Katrin Reimann; Kruthika Thangavelu
Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital Marburg, Germany.
*Corresponding Author : Nermin Abozenah
Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital Marburg, Germany.
Email: tonermin-hamdy@hotmail.com
Received : May 28, 2024
Accepted : Jul 08, 2024
Published : Jul 15, 2024
Archived : www.jcimcr.org
Copyright : © Abozenah N (2024).
Abstract
Background: Small cell neuroendocrine carcinoma is a rare malignancy that mainly affects the pulmonary tract and only occurs extrapulmonary in very few cases, accounting to about 2.5-5% of all cases [1,2]. Primary sinonasal neuroendocrine carcinoma is extremely rare and typically affects the ethmoid or maxillary sinuses, with or without concomitant involvement of the nasal cavity [3]. There are no specific risk factors predisposing to these tumors, but several common factors have been found to cluster in affected populations, including male preponderance and an average age of onset of around 50 years [4]. Due to the rarity of this disease, there are still many discrepancies regarding how to diagnose and treat these tumors and to date there are no specific recommendations regarding an optimal treatment plan.
Case overview: We present the case of a female patient diagnosed with small cell neuroendocrine carcinoma of the nasal cavity and right ethmoid sinus and explain the approach we undertook with her starting at her initial presentation in our outpatient clinic up to her diagnosis and the treatment plan we devised.
Conclusion: Due to the rarity of primary small cell neuroendocrine tumors of the paranasal sinuses, various diagnostic and therapeutic modalities are still under investigation. One common factor between the diverse applied modalities in diagnosing and treating this rare entity is that the current applied concept are derived from lung tumors of the same histological origin, given that the similar morphology of small cell neuroendocrine tumors of the paranasal sinuses and those occurring in the lung [5].
Citation: Abozenah N, Stuck BA, Boirk R, Reimann K, Thangavelu K. Insights from a unique presentation of small cell neuroendocrine carcinoma of the paranasal sinuses: A case report. J Clin Images Med Case Rep. 2024; 5(7): 3168.
Introduction
Sinonasal neuroendocrine carcinoma was first described in 1982 [5]. Since then, this disease entity remains poorly understood and very unclear. Given the rarity of its occurrence, understanding its clinical behavior remains insufficient to efficiently combat its progression and consequently improve its treatment [2,5-8]. Small cell neuroendocrine tumors of the paranasal sinuses are usually discovered at a late stage, which further complicates their management. These tumors are highly invasive, grow rapidly and tend to infiltrate adjacent structures such as the orbit, skull base and intracranial compartment locally as well as metastasize early in the course of the disease [2]. The nasal cavity is most commonly affected, followed by the ethmoid and maxillary sinuses [4]. The most common symptoms include nasal obstruction, epistaxis [4], facial swelling, localized pain and deterioration of vision [2]. However, these symptoms are not disease specific, leading to further delay in diagnosis and treatment [2]. Radiological modalities play a crucial role in the diagnosis and treatment planning of small cell neuroendocrine sinonasal carcinoma [7]. Modern radiology used in the diagnosis of this tumor type includes diffusion-weighted MRI and dynamic contrast-enhanced MRI [7]. Given the highly aggressive nature of small cell neuroendocrine tumors, a precise diagnosis must be made in order to assess the extent of the disease and plan a promising treatment. Several treatment options have been described, including surgical resection, chemotherapy, radiotherapy and a combination of two or more of these options [8]. Although responsive to local therapy, small cell neuroendocrine tumors are unfortunately associated with a high rate of local recurrence and new distant metastases [6]. Therefore, a multidisciplinary therapeutic approach must be adopted to optimize the prognosis, as current evidence has shown a poor overall survival rate with an overall 5-year survival rate of as low as 13% [1]. Considering the rarity of this condition and the lack of treatment guidelines, we present a case of primary small cell neuroendocrine tumor of the paranasal sinuses and describe the diagnostic modalities and therapeutic options we used in order to add to the database currently available in the literature.
Discussion
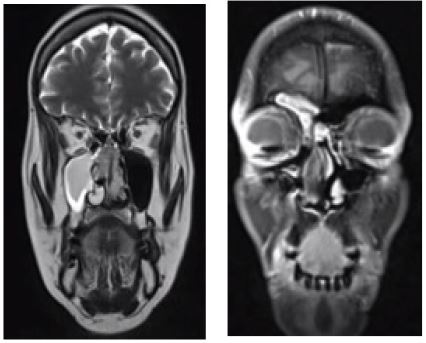
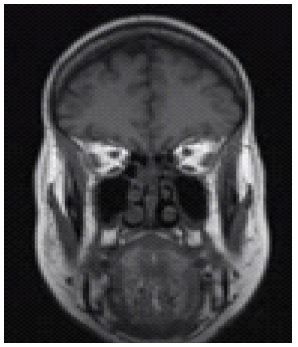
A 56-year-old female patient presented to our outpatient clinic with swelling over the nose that had been progressive for 2 years, associated with accompanying redness of the overlying skin. The patient reported severe endonasal crusting, which had been accompanied by bloody nasal secretions for about 4 months. A previous clinical presentation of the patient at another institution could not disclose any underlying pathology accounting for the patient’s signs and symptoms. A CT scan of the paranasal sinuses performed in March 2020 revealed a tumorous structure in the right ethmoid sinus with infiltration of the right nasal cavity. As the patient presented in a rather early phase of the Covid-19 pandemic, our clinical examination could only be focused in accordance with our hospital’s guidelines at the time. During the endonasal endoscopic examination, we identified a yellow, coarse tumorous structure with vascular injections. Further radiological imaging showed a soft tissue dense formation with extension in the nasal cavities over the nasal septum with an associating contact to the medial and inferior nasal turbinate on both sides. Consecutively, a subtotal ipsilateral displacement of the semilunar hiatus was detected. Furthermore, the radiological study revealed a displacement of the right posterior ethmoidal cells and the right sphenoid sinuses without detectable interruption of continuity in the course of the lamina cribrosa on both sides. The biopsy of the tumorous structure confirmed a small cell neuroendocrine tumor with TTF-1 expression, which was initially presumed to be a metastasis of an undiagnosed bronchial or nasopharyngeal carcinoma. A CT scan of the thorax ruled out a primary lung tumor and other suspicious lesions. In order to provide the patient with optimal care, the case was discussed in our interdisciplinary head and neck tumor board. Finally, induction chemotherapy with 3 cycles of cisplatin/etoposide followed by combined radiochemotherapy was decided as best point of care for the patient and the patient was referred to the haemato-oncology department for initiation of the planned therapy. The patient was declared tumor-free at 5- month and 17-month post-treatment checkups, after which the patient died of most likely a sudden cardiac arrest in April 2022, 2 years after the initial tumor diagnosis.
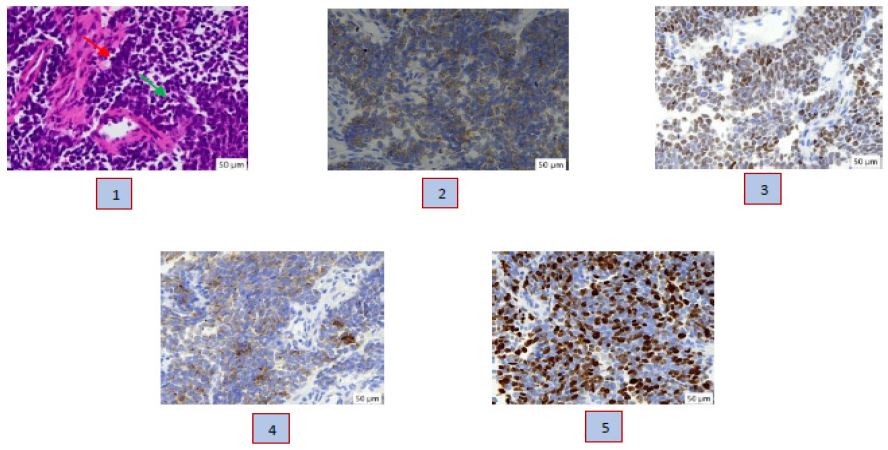
2. Synaptophysin (400x magnified): granular positive
3. TTF1 (400x magnified): nuclear positive
4. CKMNF116 (400x magnified): granular positive
5. Proliferation-Marker Ki-67 (400x magnified): 60% nuclear positive
Image source (histological demonstrations 1-5): Institute for pathology, University Hospital Marburg. Images used with permission from Dr. Fiona Rodepeter - consultant pathologist, University Hospital Marburg.
Discussion
Small cell neuroendocrine tumors are exceptionally rare, aggressive lesions that only occur extra-pulmonary in counted cases. Due to its sporadic occurrence in the nasal cavities and paranasal sinuses, this entity remains poorly understood. When arising in the nasal cavity and paranasal sinuses, these tumors show a very aggressive local infiltration rate without early metastasis in comparison to small cell neuroendocrine tumors of the lung [9]. Radiological imaging is crucial to determine the extent of the disease and particularly important for preoperative planning [10], making it one of the mainstays in the diagnosis and treatment planning of small cell neuroendocrine tumors. Surgery followed by radiotherapy or a combination of radiotherapy and chemotherapy are appropriate treatment options [9,10]. However, radiotherapy has shown to be more effective in treating small cell neuroendocrine tumors in other areas of the head and neck than in the nasal cavity [11]. At the University of Miami, 12 patients with non-metastatic small cell neuroendocrine tumors of the head and neck region were followed for 20 years. The results of this study showed that radiotherapy and chemotherapy can be a suitable alternative to surgery and offer a better therapeutic outcome for tumors in the parotid and tonsillar region than in the sinonasal region, where a more aggressive and radical therapeutic approach is necessary and advocated [11]. Another comprehensive study conducted in Berlin over a 10-year period has shown that multimodal therapy may be suitable for controlling disease progression and improving overall survival in patients with locoregional extrapulmonary small cell neuroendocrine tumors [12].
Conclusion
Small cell neuroendocrine sinonasal tumors remain an uncommon and unclear malignant entity with to date unclear diagnosis, no uniform classification system [13,14], high rate of local recurrence and distant metastasis at 33% and 31% respectively [15], lack of gold standard guidelines for treatment and overall poor prognosis. Treatment depends on the localization of the lesion, level of local invasion and presence or absence of metastasis. However, further scientific progress is essential to better codify these tumors and take a step closer to providing the best possible treatment for affected patients.
References
- Chapurin N, Totten DJ, Louis PC, Lewis Jr JS, Chowdhury NI, et al. Sinonasal small cell carcinoma-case series of a rare malignancy. Ear, Nose & Throat Journal. 2022; 101(6): 392-395.
- Wang J, Fan Y, Chen XD, Xue T, Chen FQ. (2021). Primary small cell carcinoma in nasal cavity and paranasal sinuses: 15 cases from a single center. Ear, Nose & Throat Journal. 2022; 01455613211049853.
- Sara C, Ismail Z, Rafi S, Tabib GEM, El AN. Primary sinonasal neuroendocrine carcinoma invading the orbit. In Endocrine Abstracts. Bioscientifica. 2023; 90.
- Chen LY, Chang SL, Lee WY. Primary small cell neuroendocrine carcinoma in the nasal cavity: A CARE-compliant case report. Medicine. 2021; 100(35).
- Nagy AA, Trombitas V, Vlad D, Albu S. Sinonasal neuroendocrine carcinoma- a case report. Romanian Journal of Rhinology. 2014; 4(14): 117-20.
- Khan M, Nizami S, Mirrakhimov AE, Maughan B, Bishop JA, et al. Primary small cell neuroendocrine carcinoma of paranasal sinuses. Case Reports in Medicine. 2014.
- Lin N, Qi M, Wang Z, Luo S, Pan Y, et al. Small cell neuroendocrine carcinoma of paranasal sinuses: radiologic features in 14 cases. Journal of Computer Assisted Tomography. 2021; 45(1): 135.
- Kichloo A, Parikh A, Mankada S, Suryanarayana U. Small-cell carcinoma of nasal cavity and approach to its management: A case report. Journal of Current Oncology. 2019; 2(2): 74.
- Villarreal IM, Arellano B, Pinilla M, Tejerina E, López-Cortijo C. Small-cell neuroendocrine carcinoma of the nasal septum: unusual location for a known type of neoplasm. Acta Oto-Laryngologica Case Reports. 2016; 1(1): 63-66.
- Tang IP, Singh S, Krishnan G, Looi LM. Small cell neuroendocrine carcinoma of the nasal cavity and paranasal sinuses: a rare case. The Journal of Laryngology & Otology. 2012; 126(12): 1284-1286.
- Hatoum GF, Patton B, Takita C, Abdel-Wahab M, LaFave K, et al. Small cell carcinoma of the head and neck: the university of Miami experience. International Journal of Radiation Oncology Biology Physics. 2009; 74(2): 477-481.
- Ochsenreither S, Marnitz-Schultze S, Schneider A, Koehler C, Daum S, et al. Extra pulmonary small cell carcinoma (EPSCC): 10 years’ multi- disciplinary experience at Charité. Anticancer research. 2009; 29(8): 3411-3415.
- Rindi G, Klimstra DS, Abedi-Ardekani B, Asa SL, Bosman FT, et al. A common classification framework for neuroendocrine neoplasms: an International Agency for Research on Cancer (IARC) and World Health Organization (WHO) expert consensus proposal. Modern Pathology. 2018; 31(12): 1770-1786.
- Rindi G, Mete O, Uccella S, et al. Overview of the WHO Classification of Neuroendocrine Neoplasms. Endocr Pathol. 2022; 33: 115-154. https://doi.org/10.1007/s12022-022-09708-2.
- Han G, Wang Z, Guo X, Wang M, Wu H, et al. Extrapulmonary small cell neuroendocrine carcinoma of the paranasal sinuses: A case report and review of the literature. J Oral Maxillofac Surg. 2012; 70: 2347-51.