
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Desmoid fibromatosis tumor of the buttock, mimicking a man face on MRI
Said Hilmani*; Khadija Ibahioin; Abdelhakim Lakhdar
Neurosurgical Department and Laboratory of Research on Neurology, Neurosensorial Diseases and Disability, Faculty of Medicine, Hassan II University, Ibn Rushd UHC Casablanca, Morocco.
*Corresponding Author : Said Hilmani
Neurosurgical Department and Laboratory of Research on Neurology, Neurosensorial Diseases and Disability, Faculty of Medicine, Hassan II University, IBN Rushd UHC Casablanca, Morocco.
Email: hilmani.said@yahoo.fr
Received : May 24, 2024
Accepted : Jul 08, 2024
Published : Jul 15, 2024
Archived : www.jcimcr.org
Copyright : © Hilmani S (2024).
Abstract
Purpose: Desmoid-type Fibromatosis (DF) is a rare and locally aggressive tumor that occurs predominantly between puberty and 40 years, with female predominance. The aim is to clarify the DF management.
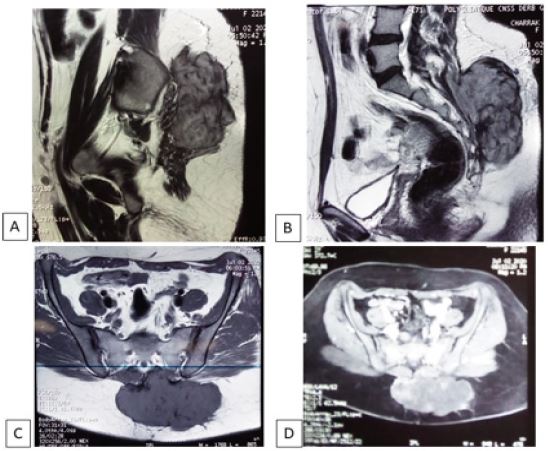
Cases report: A 30-year-old woman who had a large desmoid fibromatosis tumor of here left buttock with 2 years history of local pain. MRI showed a well defined and lobulated tumor mimicking a man face. She underwent en bloc resection of the tumor without recurrence.
Conclusion: The challenge in DF management lies not on diagnosis, but in the high frequency of recurrences that can be minimized by a carcinological resection with healthy margins, associated to close and long follow-up.
Keywords: Desmoid fibromatosis; Buttock; Musculoaponeurotic fibromatosis; En bloc resection; Recurrences.
Citation: Hilmani S, Ibahioin K, Lakhdar A. Desmoid fibromatosis tumor of the buttock, mimicking a man face on MRI. J Clin Images Med Case Rep. 2024; 5(7): 3169.
Background
Desmoid Fibromatosis tumor (DF) is a rare tumor of deep musculoaponeurotic origin, that account for 0.03% of all neoplasms and develops commonly between the age of 15 and 60 years [1]. It affects abdominal area in general with female predominance. Other less common sites are affected including buttock (sacrococcygeal region) that occur as sporadic cases, but it may have an association with genetic predisposition [2,3]. We report a rare case of a 30-year-old woman who had a large desmoid fibromatosis tumor of here right buttock, with en bloc resection.
Case presentation
A 30 year-old woman with 2 years history and 16 months after his last pregnancy, of progressive growth tumefaction of the left buttock and local pain without sciatica or neurological deficit. The patient had difficulties in walking. Clinical exam revealed a firm large mass of the right buttock, fixed to deep plane. There was no other lesion in the body. On MRI, the tumor showed a heterogeneous and isointense aspect in both T1-weighted and T2-weighted appearance, relatively well defined, with an irregular and lobulated contour. After contrast injection, the mass showed heterogeneous enhancement (Figure 1). En bloc resection of the tumor was done after a painful dissection. It was attached to deep muscle aponeurosis, with respect of sacrum bone. The excised mass was firm to hard, reddish-gray aspect, that measured approximately 14 x 6 x 4 cm (Figure 2). Surgical margins of resected specimen were free of tumor. Histopathology study confirmed the diagnosis of desmoid fibromatosis tumor. The post-operative period was uneventful with improvement in pain and walking. No adjuvant therapy was administered. One year after she developed two recurrences six month between them. The patient is under close follow-up and no recurrence is noted after two years.

Discussion
According to the World Health Organization [4], desmoid-type Fibromatosis (DF) is a rare infiltrative and locally aggressive tumors arising from musculoaponeurotic tissues. Despite that it’s histologically benign and slow-growing tumors, DF, also known as aggressive fibromatosis, has a high rate of local recurrence [5,3,6]. Enzinger and Weiss [7] had classified DF into superficial and deep (extra-abdominal and intra-abdominal) types. DF usually affects the abdominal wall but may be also found in other less common sites including sacrococcygeal region which is a rare location [2] and approximately 5-10% arises in the context of Familial Adenomatous Polyposis (FAP) and forms the Gardner syndrome [8]. If the etiopathogenesis is not unclear, some risque factors are advocated as trauma, oral contraceptives and pregnancy as shown at our patient.
Clinical diagnosis is not specific, but MRI imaging is very suggestive. The signal, size and form are variable, depending on cellular components, collagen fibers density and vascularity. Generally, DF appears a well circumscribed mass, equisignal on T1-WI and T2-WI with contrast enhancement. The lobulated shape in particular region, may give some morphotype aspect, like face, as showed in our case. At our Knowledge, the morphotype aspect of tumors, at any location, was never reported. We think that is only a coincidence. MRI is also helpful on patient management and surgical decision. Surgery is the treatment of choise. Total removal of the tumor, whenever possible, is the key of success. Thereby, the reliable indicators is en bloc resection and free margins of the tumor, without comprimising surrounding major structures and function. In this vision, Salas S et al [9], as others, report in their study about 426 cases DF, including 22 buttock location, that surgical margins do not consistently correlate with recurrence. But, local recurrences are common in incomplete resection cases, about 40% [10]. In addition and in difference to pediatric patients [11], age, site and size of the tumor are unreliable indicators for recurrence in adults. Radiotherapy has been used for local recurrence as well as those that could be excised only sub-totally, which improve the rate of local control [12]. But after complete resection, regardless of resection margins, post operative radiation is not recommended and has not demonstrated a clear benefit [5,14]. Chemotherapy, such as tamoxifen or nonsteroidal antiinflammatory drugs, have been used in cases of recurrences, unresectable tumors and for patients that are not able to surgery or radiation therapy. It with seem provide relative activity and long-term clinical benefits [15]. Spontaneous regressions, at all sites, are observed in 20%-30% of cases [9]. Accordingly, « Wait and see » approach may be reasonable in asymptomatic and low size or low growing tumors.
Conclusion
The diagnosis of the desmoids tumors is relatively easy on MRI and histologically. The problem lies in the high frequency of recurrences that can be minimized by a carcinological resection with healthy margins. If invaded margins and partially resection, an external radiotherapy and a long follow-up are necessary.
References
- Sakorafas GH, Nissotakis C, Peros G. Abdominal desmoid tumors. Surg Oncol. 2007; 16:131-142.
- Pan F, Liu Q, Zhang G, Wang Q, Yun B, et al. Aggressive fibromatosis of the leg and sacrococcygeal region: A report of two cases. Int J Clin Exp Pathol. 2015; 8(1): 948-53.
- Sarin YK, Khurana N. Desmoid tumor of the buttock in a preadolescent child. .APSP J Case Rep. 2011; 2(1): 2.
- Fletcher CDM, Bridge JA, Hogendoorn P, Mertens F, WHO Classification of Tumours of Soft Tissue and Bone; 4th edition, Lyon: IARC. 2013.
- Kasper BC, Baumgarten J, Garcia S, Bonvalot R, Haas F, et al. Gronchi, On behalf of the Desmoid Working Group. An update on the management of sporadic desmoid-type fibromatosis: A European Consensus Initiative between Sarcoma Patients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG); Annals of Oncology. 2017; 28: 2399-2408. doi:10.1093/annonc/mdx323, Published online 23 June 2017.
- Penel N, Coindre JM, Bonvalot S, et al. Management of desmoid tumours: A nationwide survey of labelled reference centre networks in France. Eur J Cancer 2016; 58: 90-96.
- Enzinger FM, Weiss SW. Soft tissue tumors, 3rd ed. St. Louis: Mosby.1995; 165-268.
- Gardner EJ. A genetic and clinical study of intestinal polyposis, a predisposing factor for carcinoma of the colon and rectum. Am J Hum Genet 1951; 3: 167-76.
- Ganeshan D, Amini B, Nikolaidis P, Assing M, Vikram R. Current Update on Desmoid Fibromatosis. J Comput Assist Tomogr. 2019; 43(1): 29-38.
- Wang YF, Guo W, Sun KK, et al. Postoperative recurrence of desmoid tumors: Clinical and pathological perspectives. World J Surg Oncol. 2015; 13: 26.
- Salas S, Dufresne A, Bui B, et al. Prognostic factors influencing progression-free survival determined from a series of sporadic desmoid tumors: a wait-and-see policy according to tumor presentation. J Clin Oncol. 2011; 29: 3553-3558.
- Ning B, Jian N, Ma R. Clinical prognostic factors for pediatric extra-bdominal desmoid tumor: analyses of 66 patients at a single institution. World J Surg Oncol. 2018; 16(1): 237.
- Atahan IL, Akyol F, Zorlu F, Gurkaynak M. Radiotherapy in the management of aggressive fibromatosis. Br J Radiol. 1989; 62: 854-6.
- Okuno SH, Edmonson JH. Cancer. Combination chemotherapy for desmoid tumors. 2003; 97(4): 1134-5. doi: 10.1002/cncr.11189.
- Roussin S, Mazouni C, Rimareix F, et al. Toward a new strategy in desmoid of the breast? Eur J Surg Oncol 2015; 41: 571-576.